| 1) Holroyd KA, Penzien DB, Cordingley GE: Propranolol in the management of recurrent migraine: a meta-analytic review. Headache 1991; 31(5): 333-340. |
文献(ABフォーム)ID
|
1
|
文献PubMed−ID
|
PMID:1830566
|
文献タイトル(日本語)
|
再発性片頭痛管理におけるプロプラノロール:メタ解析レビュー
|
文献タイトル(英語)
|
Propranolol
in the management of recurrent migraine: a meta-analytic review.
|
エビデンスレベル
|
Ia
|
著者名
|
Holroyd,K.A.;
Penzien,D.B.; Cordingley,G.E.
|
雑誌名,出版年 巻: 頁
|
Headache. 1991; 31: 333-40
|
目的
|
β遮断薬プロプラノロールの片頭痛予防療法を評価した研究から有効性を検索する.
|
研究デザイン
|
Meta-analysis
|
研究施設
|
|
研究期間
|
|
対象患者
|
53の臨床試験(プロプラノロールで治療された片頭痛患者2403人)
|
介入
|
Medlineなどの医学文献分析検索システム・データベースで成人片頭痛患者でプロプラノロールで治療された5症例以上の報告,片頭痛改善の度合いを表したものがあるものをコンピューター検索した.
|
主要評価項目とそれに用いた統計学的手法
|
頭痛治療インデックス(H.I.)を治療前vs.プロプラノロール,プロプラノロールvs.プラセボ,プラセボvs.プロプラノロールで算出した.
|
結果
|
プロプラノロール典型的な投与量は160mg/日であった.
二重盲検試験でのプロプラノロール有効率は平均43.7%で,プラセボの有効率14.3%より有意に高値(p<0.001)であった.
頭痛日記を用いた評価ではプロプラノロールは片頭痛発作を44%減少させた.古典的な患者の自覚的改善度や臨床的な有効性で評価するとプロプラノロールは片頭痛を65%改善させた.プラセボではいずれの評価法でも約14%の片頭痛改善を認めた.
研究により投与量が異なっているが,投与量と片頭痛予防効果の用量-反応関係は明確ではなかった.
プロプラノロールの認容性は良好であった.
|
結論
|
β遮断薬プロプラノロールの片頭痛予防薬としての効果は確実である
|
作成者
|
井尻珠美/竹島多賀夫
|
コメント-1
|
研究およびレポートの質は高い.ただし,解析対象の研究報告は古いものが多く現在の基準からは不完全な臨床試験を対象としたメタアナリシスである.
|
コメント-2
|
|
備考1
|
Publication
Types:
- Clinical Trial
- Meta-Analysis
MeSH Terms:
- Adult
- Female
- Human
- Male
- Meta-Analysis
- Migraine/drug
therapy*
- Migraine/physiopathology
- Migraine/prevention
& control
- Prognosis
- Propranolol/adverse
effects
- Propranolol/therapeutic
use*
- Recurrence
Substances:
|
備考2
|
hed_3105333.pdf
|
備考3
|
|
論文抄録
|
We used meta-analytic statistical
techniques to synthesize findings from studies that evaluated propranolol HCI
for the prevention of recurrent migraine (2,403 treated patients). The modal
migraine sufferer treated in these studies was a female, about 37 years of
age, who suffered from common (rather than classical) migraines and reported
a 17-year history of problem migraines. The modal treatment was 160mg.
propranolol per day. Meta-analysis revealed that, on average, propranolol
yielded a 44% reduction in migraine activity when daily headache recordings
were used to assess treatment outcome, and a 65% reduction in migraine
activity when less conservative measures (e.g., clinical ratings of
improvement, global patient reports) were used. Meta-analysis thus revealed
substantial support for short-term effectiveness of propranolol. However,
little information was available concerning the long-term effectiveness of
propranolol.
|
|
| |
| 2) Holland S, Silberstein SD, Freitag F, Dodick DW, Argoff C, Ashman E. Correspondence & reprint requests to American Academy of Neurology Evidence-based guideline update: NSAIDs and other complementary treatments for episodic migraine prevention in adults: Report of the Quality Standards Subcommittee of the American Academy of Neurology and the American Headache Society. Neurology. 2012;78(17):1346-53. |
文献(ABフォーム)ID
|
2
|
文献PubMed−ID
|
PMID: 22529203
|
文献タイトル(日本語)
|
|
文献タイトル(英語)
|
Evidence-based guideline update: NSAIDs and other complementary treatments for episodic migraine prevention in adults: Report of the Quality
Standards Subcommittee of the American Academy of Neurology and the American
Headache Society.
|
エビデンスレベル
|
|
著者名
|
Holland
S, Silberstein SD, Freitag F, Dodick DW, Argoff C, Ashman E.
Correspondence & reprint
requests to American Academy of Neurology
|
雑誌名,出版年 巻: 頁
|
Neurology.
2012 Apr 24;78(17):1346-53.
|
目的
|
|
研究デザイン
|
|
研究施設
|
|
研究期間
|
June 1999 to May
2009
|
対象患者
|
|
介入
|
|
主要評価項目とそれに用いた統計学的手法
|
|
結果
|
284 abstracts
|
結論
|
|
作成者
|
|
コメント-1
|
|
コメント-2
|
|
備考1
|
|
備考2
|
|
備考3
|
|
備考4
|
|
論文抄録
|
OBJECTIVE:
To provide updated evidence-based recommendations for the preventive
treatment of migraine headache. The clinical question addressed was: Are
nonsteroidal anti-inflammatory drugs (NSAIDs) or other complementary
treatments effective for migraine prevention?
METHODS:
The authors analyzed published studies from June 1999 to May 2009 using a
structured review process to classify the evidence relative to the efficacy
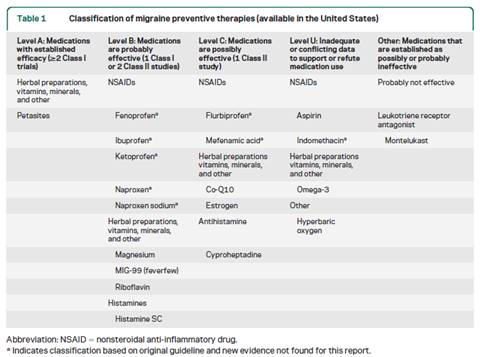
of various medications for migraine prevention. RESULTS: The author panel
reviewed 284 abstracts, which ultimately yielded 49 Class I or Class II
articles on migraine prevention; of these 49, 15 were classified as involving
nontraditional therapies, NSAIDs, and other complementary therapies that are
reviewed herein. Recommendations: Petasites (butterbur) is effective for migraine
prevention and should be offered to patients with migraine to reduce the
frequency and severity of migraine attacks (Level A). Fenoprofen, ibuprofen,
ketoprofen, naproxen, naproxen sodium, MIG-99 (feverfew), magnesium,
riboflavin, and subcutaneous histamine are probably effective for migraine
prevention (Level B). Treatments considered possibly effective are
cyproheptadine, Co-Q10, estrogen, mefenamic acid, and flurbiprofen (Level C).
Data are conflicting or inadequate to support or refute use of aspirin,
indomethacin, omega-3, or hyperbaric oxygen for migraine prevention.
Montelukast is established as
probably ineffective for migraine prevention (Level B).
|
|
| |
| 3) Silberstein SD, Holland S, Freitag F, Dodick DW, Argoff C, Ashman E. Evidence-based guideline update: Pharmacologic treatment for episodic migraine prevention in adults: Report of the Quality Standards Subcommittee of the American Academy of Neurology and the American Headache Society. Neurology. 2012; 78(17): 1337-1345. |
文献(ABフォーム)ID
|
3
|
文献PubMed−ID
|
PMID:
22529202
|
文献タイトル(日本語)
|
|
文献タイトル(英語)
|
Evidence-based guideline update:
Pharmacologic treatment for episodic migraine prevention in adults: Report of
the Quality Standards Subcommittee of the American Academy of Neurology and
the American Headache Society.
|
エビデンスレベル
|
|
著者名
|
Silberstein SD, Holland S, Freitag F,
Dodick DW, Argoff C, Ashman E.
Correspondence & reprint requests to American
Academy of Neurology
|
雑誌名,出版年 巻: 頁
|
Neurology. 2012 Apr 24; 78(17):
1337-1345
|
目的
|
|
研究デザイン
|
|
研究施設
|
|
研究期間
|
|
対象患者
|
|
介入
|
|
主要評価項目とそれに用いた統計学的手法
|
|
結果
|
|
結論
|
|
作成者
|
|
コメント-1
|
|
コメント-2
|
|
備考1
|
|
備考2
|
|
備考3
|
|
備考4
|
|
論文抄録
|
OBJECTIVE: To provide updated
evidence-based recommendations for the preventive treatment of migraine
headache. The clinical question addressed was: What pharmacologic therapies
are proven effective for migraine prevention?
METHODS: The authors analyzed
published studies from June 1999 to May 2009 using a structured review
process to classify the evidence relative to the efficacy of various
medications available in the United States for migraine prevention. Results
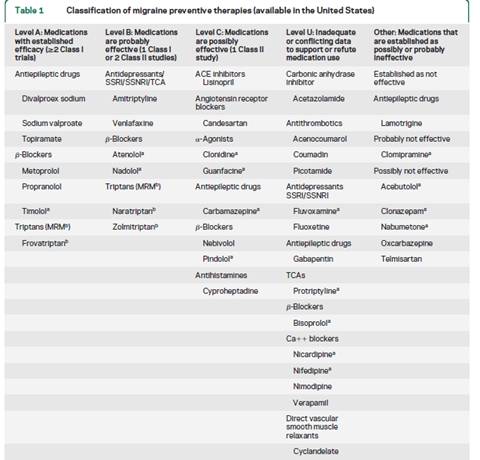
and Recommendations: The author panel reviewed 284 abstracts, which
ultimately yielded 29 Class I or Class II articles that are reviewed herein.
Divalproex sodium, sodium valproate, topiramate, metoprolol, propranolol, and
timolol are effective for migraine prevention and should be offered to
patients with migraine to reduce migraine attack frequency and severity
(Level A). Frovatriptan is effective for prevention of menstrual migraine
(Level A). Lamotrigine is ineffective for migraine prevention (Level A).
|
|
| |
4) Silberstein SD: Practice parameter: evidence-based guidelines for migraine headache (an evidence-based review): report of the Quality
Standards Subcommittee of the American Academy of Neurology. Neurology 2000; 55(6): 754-762. |
文献(ABフォーム)ID
|
4
|
文献PubMed−ID
|
PMID: 10993991
|
文献タイトル(日本語)
|
実地臨床パラメーター:片頭痛のエビデンスに基づくガイドライン
|
文献タイトル(英語)
|
Practice parameter:
evidence-based guidelines for migraine headache (an evidence-based review):
report of the Quality Standards Subcommittee of the American Academy of
Neurology.
|
エビデンスレベル
|
N/A
|
著者名
|
Silberstein SD.
|
雑誌名,出版年 巻: 頁
|
Neurology 2000; 55(6):
754-762.
|
目的
|
N/A
|
研究デザイン
|
4件のEBMによる片頭痛患者のマネージメントに関するレビュー1)急性期治療,2)予防療法,3)非薬物療法,4)画像検査をもとに主要な治療の勧告のみを記述.
|
研究施設
|
N/A
|
研究期間
|
N/A
|
対象患者
|
N/A
|
介入
|
N/A
|
主要評価項目とそれに用いた統計学的手法
|
N/A
|
結果
|
臨床的疑問
作成のプロセス
エビデンスの解析
片頭痛の診断
片頭痛の治療
片頭痛の急性期治療
片頭痛の予防療法
---
片頭痛予防療法の目的(ゴール):
1) 発作頻度,重症度と頭痛持続時間の軽;
2) 急性期治療の反応の改善
3)生活機能の向上と,生活への支障の軽減.
以下の項目があれば予防治療の使用を考慮する.
·
急性期の治療をしても,片頭痛発作により日常生活に支障がある場合(患者の意見による頻繁な頭痛)
·
急性期治療薬が禁忌,あるいは無効,または急性治療薬の乱用がある,急性治療による有害事象
·
急性期治療と予防療法の費用バランス
·
患者の選択(嗜好)
·
片麻痺性片頭痛,脳底片頭痛,遷延性前兆を伴う片頭痛,または片頭痛梗塞などまれな片頭痛状況の存在(神経障害の予防が必要.専門家のコンセンサスに基づく)
これらのコンセンサスに基づく片頭痛ケアの原則に従えば,予防療法が成功する可能性が高くなる.
非薬物治療も考慮すること.また,患者の選択(嗜好)も考慮が必要.
1. 薬物投与使用:
A.エビデンス基づいた有効性が最も高いレベルにある薬物の投与から予防療法を始める.
B.最低用量から開始して,有害事象が無い限り,十分な臨床効果が得られる用量までゆっくり増量する.
C.各薬剤の効果判定を十分に行う必要がある.通常,臨床効果を達成するまでに2〜3ヵ月かかる可能性がある.
D.有害な薬物使用(例えば急性期治療薬の濫用)を回避する.
E.長時間作用型の製剤は,コンプライアンスを改善する可能性がある.
2. 評価:
A.頭痛日記を通して患者の頭痛をモニタする.
B.治療の再評価:3〜6ヵ月後に頭痛がかなりよくコントロールされている場合,治療の漸減または,中止を考慮する.
3. 併存する医学的状態を考慮する.
いくつかの(併存症/共存しているcomorbid/coexisting)状態は,片頭痛患者において一般的である:脳卒中,心筋梗塞,Raynaud’s現象,てんかん,情動性および不安性疾患.これらの存在は,治療の機会と限界の双方に関与する.
A.可能ならば,併存症と片頭痛の双方を治療できる薬を選択する.
B.片頭痛のために使用する治療薬は,併存疾患の禁忌でないものを選択する.
C.併存症の治療に使用される薬剤は片頭痛を悪化させないものを選択する.
D.全ての薬物相互作用にも注意する.
4. 妊婦または妊娠希望の女性に対する留意点
予防的な薬物投与は,催奇形作用を持つ可能性がある.
予防療法が不可欠の場合,胎児に対するリスクが最も低い薬剤を選択する.
5. 多くの片頭痛患者は頭痛のコントロールの目的で,薬物療法の開始前,あるいは,薬物療法と同時に,非薬物療法を試みようとするものである.行動療法(Behavioral
treatments)は,3つのカテゴリーに大別できる:リラクセーション・トレーニング,バイオ・フィードバック療法,および,認知行動療法(ストレス対策トレーニング)である.
理学療法には,鍼,ervical manipulation, およびmobilization
therapyが含まれる.これらは,以下のような頭痛患者のための治療オプションである:
A.非薬物療法を好む患者
B.特異的な薬物療法に耐えれない患者
C.特異的な薬物療法が禁忌である場合
D.薬物療法に反応しない患者
E.妊婦,妊娠希望婦人,授乳婦
F.頭痛を悪化させたり,(他の薬物療法への反応性の低下を誘導する)鎮痛剤や他の急性期治療薬の長期にわたる,頻用,過剰使用のある患者(または薬剤)
G.明らかなストレス下にある患者,またはストレスのコーピング能力が不十分な患者
|
結論
|
N/A
|
作成者
|
竹島多賀夫
|
コメント-1
|
米国の片頭痛診療ガイドライン.2000年,EBMを主体にしてコンセンサスを取り入れたガイドライン.
|
コメント-2
|
|
備考1
|
Neurology55754.pdf
|
備考2
|
DA
- 20001004
IS
- 0028-3878
LA
- eng
PT
- Guideline
PT
- Journal Article
PT
- Practice Guideline
SB -
AIM
SB - IM
|
備考3
|
|
備考4
|
|
論文抄録
|
|
|
| |
5) Ramadan NM, Silberstein SD, Freitag FG, Gilbert TT, Frishberg BM: Evidence-based guidelines for migraine headache:
pharmacological management for prevention of migraine. Available at:http://www.aan.com/professionals/practice/pdfs/gl0090.pdf(accessed
13 December 2011) |
文献(ABフォーム)ID
|
5
|
文献PubMed−ID
|
|
文献タイトル(日本語)
|
片頭痛のエビデンスに基づくガイドライン:片頭痛予防のための薬物療法
|
文献タイトル(英語)
|
Evidence-based
guidelines for migraine headache: pharmacological management for prevention
of migraine.
|
エビデンスレベル
|
N/A
|
著者名
|
Ramadan NM,
Silberstein SD, Freitag FG, Gilbert TT, Frishberg BM.
|
雑誌名,出版年 巻: 頁
|
Online Pub 2000.
http://www.aan.com/professionals/practice/pdfs/gl0090.pdf
|
目的
|
予防治療の有効性,耐容性と安全性の科学的なエビデンスを示す.
Guidelineには,科学的なエビデンスと臨床的経験に基づくレベルを示したエビデンスのレビュー・テーブルを含む.
科学的なエビデンスが不足する場合の,推奨された治療戦略はGuidelineを作成した米国頭痛コンソーシアムのメンバーのコンセンサスに基づく.コンセンサスは,明示しないかぎり満場一致のコンセンサスである.
|
研究デザイン
|
N/A
|
研究施設
|
N/A
|
研究期間
|
N/A
|
対象患者
|
N/A
|
介入
|
N/A
|
主要評価項目とそれに用いた統計学的手法
|
N/A
|
結果
|
·
治療ゴール
·
エビデンスサマリ
·
エビデンスからガイドラインへの移行
·
管理の原則
·
特異的治療の勧告
---
予防療法の適応
これまでの片頭痛予防療法の適応推奨は月に2回以上持つ患者とされていた.
これらの勧告は,任意であり,個々の患者ニーズや他の片頭痛性状を考慮していない.
予防療法の適応は,以下の一つ以上により,適切に導かれる可能性がある:
・急性期治療にもかかわらず,患者の意見において,有意な日常生活の阻害が繰り返されている片頭痛
・ 頻繁な頭痛,
・急性期治療が禁忌,または無効,または乱用がある場合.
・ 急性期治療による有害事象,
・ 急性期治療と予防治療の費用,
・ 患者の好み,
・ 片麻痺性片頭痛,脳底片頭痛,遷延性前兆を伴う片頭痛または片頭痛梗塞など,まれな片頭痛状況の存在 (専門家のコンセンサス:神経障害を予防するため).
予防療法のゴール
(1) 発作頻度,重症度と持続時間の軽減
(2) 急性期治療の反応性を改善
(3) 頭痛患者の機能を改善して,日常生活への支障を軽減する
|
結論
|
|
作成者
|
竹島多賀夫
|
コメント-1
|
2000年の米国頭痛コンソーシアムのエビデンスマップとエキスパートコンセンサス
|
コメント-2
|
|
備考1
|
gl0090.pdf
|
備考2
|
|
備考3
|
|
備考4
|
|
論文抄録
|
|
|
| |
| 6) Guidelines and recommendations for the treatment of migraine. Italian Society for the Study of Headache (SISC). Funct Neurol 1993; 8(6):441-446. |
文献(ABフォーム)ID
|
6
|
文献PubMed−ID
|
PMID: 8150324
|
文献タイトル(日本語)
|
片頭痛治療のガイドラインと勧告
|
文献タイトル(英語)
|
Guidelines
and recommendations for the treatment of migraine. Italian Society for the
Study of Headache (SISC).
|
エビデンスレベル
|
N/A
|
著者名
|
Italian
Society for the Study of Headache (SISC)
|
雑誌名,出版年 巻: 頁
|
Funct
Neurol 1993; 8(6):441-446.
|
目的
|
頭痛治療に関与する医師に片頭痛治療に関する最近の知見を知らせるためにSISCが作成
|
研究デザイン
|
エキスパート・コンセンサス
|
研究施設
|
Italian
Society for the Study of Headache (SISC)
|
研究期間
|
N/A
|
対象患者
|
N/A
|
介入
|
N/A
|
主要評価項目とそれに用いた統計学的手法
|
N/A
|
結果
|
●
分類と診断基準:国際頭痛学会
●
予防と治療
片頭痛治療
1.
対症療法
2.
予防療法
·
予防療法(3-6ヶ月):月2回以上の生活に支障をきたす頭痛発作.月4日以上
·
予防療法は,対症療法のみで3ヶ月経過をみてから実施する.
·
予防療法の適正な評価には,頭痛の正常や持続の観察,急性期治療薬の使用量のモニターが有用.頭痛日記(ダイアリ)が有用.単純な頭痛日数の記録だけでもかなり有用.
·
予防療法はいつまで続けるか?:最低3ヶ月
·
予防療法はいつ中止するか?:頭痛が月に1-2回以下が2ヶ月以上.
|
結論
|
N/A
|
作成者
|
竹島多賀夫
|
コメント-1
|
1993年,イタリアのガイドライン.コンセンサスによる.
|
コメント-2
|
|
備考1
|
Xeroxコピー
|
備考2
|
DA
- 19940509
IS
- 0393-5264
LA
- eng
PT
- Guideline
PT
- Journal Article
PT
- Practice Guideline
RN
- 0 (Analgesics)
RN
- 0 (Ergot Alkaloids)
RN
- 103628-46-2 (Sumatriptan)
SB
- IM
|
備考3
|
|
備考4
|
|
論文抄録
|
N/A
|
|
| |
| 7) Pryse-Phillips WE, Dodick DW, Edmeads JG, Gawel MJ, Nelson RF, Purdy RA et al. Guidelines for the diagnosis and management of migraine in clinical practice. Canadian Headache Society. CMAJ 1997; 156(9):1273-1287. |
文献(ABフォーム)ID
|
7
|
文献PubMed−ID
|
PMID: 9145054
|
文献タイトル(日本語)
|
実地臨床における片頭痛の診断と治療ガイドライン
|
文献タイトル(英語)
|
Guidelines for the
diagnosis and management of migraine in clinical practice.
|
エビデンスレベル
|
N/A
|
著者名
|
Canadian Headache
Society.
Pryse-Phillips WE,
Dodick DW, Edmeads JG, Gawel MJ, Nelson RF, Purdy RA et al.
|
雑誌名,出版年 巻: 頁
|
CMAJ 1997;
156(9):1273-1287.
|
目的
|
医師および医療従事者に片頭痛の診断と治療のガイドラインを供給する.
|
研究デザイン
|
エキスパートのコンセンサス形成カンファレンス
|
研究施設
|
カナダ頭痛学会
|
研究期間
|
N/A
|
対象患者
|
N/A
|
介入
|
N/A
|
主要評価項目とそれに用いた統計学的手法
|
N/A
|
結果
|
ガイドライン作成手順
診断
対症療法:急性期治療
予防療法:
予防的片頭痛マネージメント:
----
予防療法の目標:頭痛頻度と程度を50%以下にする.
適応: 片頭痛発作が重度でQOLが阻害される. 月に3回以上発作があり,急性期治療薬では十分対処できない.
|
結論
|
N/A
|
作成者
|
竹島多賀夫
|
コメント-1
|
1997年,カナダの片頭痛診療ガイドライン.各薬剤の使用方法が具体的に記載されている.
|
コメント-2
|
|
備考1
|
CMAJ1561273.pdf
|
備考2
|
DA - 19970603
IS - 0820-3946
LA - eng
PT - Consensus Development Conference
PT - Guideline
PT - Journal Article
PT - Practice Guideline
PT - Review
RN - 0 (Adrenergic beta-Antagonists)
RN - 0 (Analgesics)
RN - 0 (Anti-Inflammatory Agents)
RN - 0 (Calcium Channel Blockers)
RN - 0 (Serotonin Antagonists)
SB - AIM
SB - IM
|
備考3
|
|
備考4
|
|
論文抄録
|
OBJECTIVE: To provide physicians and allied health care professionals
with guidelines for the diagnosis and management of migraine in clinical
practice. OPTIONS: The full range and quality of diagnostic and therapeutic
methods available for the management of migraine. OUTCOMES: Improvement in the
diagnosis and treatment of migraine, which will lead to a reduction in
suffering, increased productivity and decreased economic burden. EVIDENCE AND
VALUES: The creation of the guidelines followed a needs assessment by members
of the Canadian Headache Society and included a statement of objectives;
development of guidelines by multidisciplinary working groups using
information from literature reviews and other resources; comparison of
alternative clinical pathways and description of how published data were
analysed; definition of the level of evidence for data in each case;
evaluation and revision of the guidelines at a consensus conference held in
Ottawa on Oct. 27-29, 1995; redrafting and insertion of tables showing key
variables and data from various studies and tables of data with
recommendations; and reassessment by all conference participants. BENEFITS,
HARMS AND COSTS: Accuracy in diagnosis is a major factor in improving
therapeutic effectiveness. Improvement in the precise diagnosis of migraine,
coupled with a rational plan for the treatment of acute attacks and for
prophylactic therapy, is likely to lead to substantial benefits in both human
and economic terms. RECOMMENDATIONS: The diagnosis of migraine can be
improved by using modified criteria of the International Headache Society as
well as a semistructured patient interview technique. Appropriate treatment
of symptoms should take into account the severity of the migraine attack,
since most patients will have attacks of differing severity and can learn to
use medication appropriate for each attack. When headaches are frequent or
particularly severe, prophylactic therapy should be considered. Both the
avoidance of migraine trigger factors and the application of
nonpharmacological therapies play important roles in overall migraine
management and will be addressed at a later date. VALIDATION: The guidelines
are based on consensus of Canadian experts in neurology, emergency medicine,
psychiatry, psychology, family medicine and pharmacology, and consumers.
Previous guidelines did not exist. Field testing of the guidelines is in
progress
|
|
| |
| 8) Guidelines for the management of headache. Danish Neurological Society and the Danish Headache Society. Cephalalgia 1998; 18(1):9-22. |
文献(ABフォーム)ID
|
8
|
文献PubMed−ID
|
PM:9601619
|
文献タイトル(日本語)
|
頭痛治療ガイドライン
|
文献タイトル(英語)
|
Guidelines for the
management of headache.
|
エビデンスレベル
|
N/A
|
著者名
|
Danish Neurological
Society and the Danish Headache Society
|
雑誌名,出版年 巻: 頁
|
Cephalalgia 1998;
18(1):9-22
|
目的
|
主要目的:頭痛診療における問題点を記載することによって,保健診療システム,医師や他の医療従事者および頭痛診療に関与するすべての関係者に,頭痛診療に関する評価の改善をもたらす.
追加的目的:医師が行うべき最小限度の標準的頭痛診療について概説する.
|
研究デザイン
|
専門家・コンセンサス
|
研究施設
|
デンマーク神経学会およびデンマーク頭痛学会
|
研究期間
|
N/A
|
対象患者
|
N/A
|
介入
|
N/A
|
主要評価項目とそれに用いた統計学的手法
|
N/A
|
結果
|
疫学
患者の診療の流れ(手順)と治療レベル
急性期治療
非急性期治療
片頭痛発作予防療法:
·
予防療法適応:急性期療法のみでは治療効果が不十分な時.通常,月に2回以上,または遷延性の発作がある場合.
·
予防療法は,発作の頻度を減らすことを目標にする;発作完全抑制を目標にしない.
·
予防療法の治療期間:6−12ヵ月行い,継続が必要かどうかを判定する.
|
結論
|
N/A
|
作成者
|
竹島多賀夫
|
コメント-1
|
デンマークの頭痛診療ガイドライン1998年版.
コンセンサスによる記述.
|
コメント-2
|
|
備考1
|
Cephalalgia18009.pdf
|
備考2
|
DA - 19980807
IS - 0333-1024
LA - eng
PT - Guideline
PT - Journal Article
PT - Practice Guideline
SB - IM
|
備考3
|
|
論文抄録
|
|
|
| |
| 9) Snow V, Weiss K, Wall EM, Mottur-Pilson C. Pharmacologic management of acute attacks of migraine and prevention of migraine headache. Ann Intern Med 2002; 137(10):840-849. |
文献(ABフォーム)ID
|
9
|
文献PubMed−ID
|
PMID: 12435222
|
文献タイトル(日本語)
|
片頭痛急性期薬物治療と予防療法
|
文献タイトル(英語)
|
Pharmacologic
management of acute attacks of migraine and prevention of migraine headache.
|
エビデンスレベル
|
N/A
|
著者名
|
Snow
V, Weiss K, Wall EM and Mottur-Pilson C, for the American Academy of Family
Physicians and the American College of Physicians–American Society of
Internal Medicine
|
雑誌名,出版年 巻: 頁
|
Ann
Intern Med. 2002; 137:840-849
|
目的
|
プライマリケア医のための片頭痛治療ガイドライン
|
研究デザイン
|
EBM + エキスパートコンセンサス
|
研究施設
|
N/A
|
研究期間
|
N/A
|
対象患者
|
N/A
|
介入
|
N/A
|
主要評価項目とそれに用いた統計学的手法
|
N/A
|
結果
|
診断
急性期治療
予防療法による片頭痛のマネージメント
推奨
----
予防療法の適応;
1)
1ヵ月につき3日以上の,生活に支障がある頭痛発作が月に2回以上
2) 急性期治療が禁忌または無効で使用できない;
3) 週2回以上の頓用薬の使用;
4) 片麻痺性片頭痛,遷延性前兆を伴う片頭痛,または片頭痛性梗塞を含むまれな片頭痛状況の存在
さらに急性期治療の副作用,患者の嗜好,急性期治療と予防治療のコストなども考慮する
推奨予防治療薬
片頭痛予防の第一選択として,プロプラノロール(80〜240mg/d),チモロール(20〜30mg/d),アミトリプチリン(30〜150mg/d),divalproexナトリウム(500〜1500mg/d),バルプロ酸ナトリウム(800〜1500mg/d)が推奨できる.
フルナリジン,リスリド,ピゾチフェン,timereleased-DHE,メチセルジドは,有効性は証明されているが,有害事象に関するデータが不十分か,あるいは,頻繁ないし重度の有害事象がおこりうる薬剤である.
|
結論
|
N/A
|
作成者
|
竹島多賀夫
|
コメント-1
|
米国内科学会のガイドライン.2002年.
2000年の米国頭痛コンソーシアム(Silberstein)のガイドラインをふまえて,プライマリケア医むけに記述されている.
|
コメント-2
|
|
備考1
|
AnnIntMed137840.pdf
|
備考2
|
DA
- 20021118
IS
- 1539-3704
LA
- eng
PT
- Guideline
PT
- Journal Article
PT
- Practice Guideline
PT
- Review
PT
- Review, Academic
RN
- 0 (Adrenergic beta-Antagonists)
RN
- 0 (Anti-Inflammatory Agents, Non-Steroidal)
RN
- 0 (Anticonvulsants)
RN
- 0 (Antidepressive Agents)
RN
- 0 (Calcium Channel Blockers)
RN
- 0 (Ergotamines)
RN
- 0 (Narcotics)
RN
- 0 (Serotonin Agonists)
SB -
AIM
SB - IM
|
備考3
|
|
論文抄録
|
|
|
| |
| 10) Geraud G, Lanteri-Minet M, Lucas C, Valade D. French guidelines for the diagnosis and management of migraine in adults and children. Clin Ther 2004; 26(8):1305-1318. |
文献(ABフォーム)ID
|
10
|
文献PubMed−ID
|
PMID: 15476911
|
文献タイトル(日本語)
|
成人および小児片頭痛患者の診断とマネージメントのためのフランス・ガイドライン
|
文献タイトル(英語)
|
French guidelines for the diagnosis and management of migraine in adults
and children.
|
エビデンスレベル
|
N/A
|
著者名
|
Geraud G, Lanteri-Minet M, Lucas C, Valade D.
|
雑誌名,出版年 巻: 頁
|
Clin Ther 2004; 26(8):1305-1318.
|
目的
|
本論文は成人と小児に適用するガイドライン要約であり,
フランスにおける片頭痛患者の最適治療をめざすためのステップと方向性を提案するものである
|
研究デザイン
|
勧告は,National Agency for
Accreditation and Evaluation in Health (ANAES)の方法により3段階のレベル(A - C)に分類し,ANAESのWorking GroupメンバーとGuidelines Review
Group内の専門的コンセンサスに基づいた.
|
研究施設
|
N/A
|
研究期間
|
N/A
|
対象患者
|
N/A
|
介入
|
N/A
|
主要評価項目とそれに用いた統計学的手法
|
N/A
|
結果
|
片頭痛(成人)
有病率
臨床診断:IHS基準
片頭痛マネージメントを最適化するための障害評価方法
急性期治療
予防療法
治療ストラテジー
小児片頭痛
-----
予防療法の開始時期:
(1) 片頭痛発作の頻度や程度と片頭痛発作によるADL障害があるとき.
(2) 3ヶ月以上にわたり,毎月6−8回の急性期治療薬を使用している場合.
治療開始
単剤,低用量から開始.副作用も勘案し最適な用量まで徐々に増量する.
予防療法の有効性評価
片頭痛予防療法の有効性は治療3ヵ月以降に評価する.
片頭痛の発作頻度が50%以下になれば,治療は有効と考えてよい.
また,急性治療薬の使用量と,日記から,片頭痛発作の重症度と持続時間の減少も考慮する.
予防療法が無効の場合,副作用が無ければ増量するか,他の薬剤を試みる.
各々の単独療法を検討した後に,副作用の軽減のために低用量で,複数の薬剤の併用療法を検討してみる.
予防療法の中止・中断
奏功した場合,予防療法は6ヶ月〜1年は継続する必要がある.
その後,3-6ヵ月以上かけて漸減する.発作の頻度が再び増加する場合は同じ治療を再開する.
|
結論
|
このガイドラインは,一般開業医がエビデンスに基づく医学の原則に従った片頭痛患者管理の実践を支援するものである.
|
作成者
|
竹島多賀夫
|
コメント-1
|
2004年,フランスのガイドライン.エビデンス+コンセンサス
|
コメント-2
|
|
備考1
|
ClinTher261305.pdf
|
備考2
|
DA - 20041012
IS - 0149-2918
LA - eng
PT - Guideline
PT - Journal Article
PT - Practice Guideline
RN - 0 (Analgesics)
RN - 0 (Antidepressive
Agents)
RN - 0 (Vasoconstrictor
Agents)
SB - IM
|
備考3
|
|
備考4
|
|
論文抄録
|
BACKGROUND: The French Recommendations for Clinical Practice: Diagnosis
and Therapy of Migraine are guidelines concerning the overall management of
patients with migraine, including diagnostic and therapeutic strategies and
assessment of disability. OBJECTIVE: This article summarizes the guidelines
as they apply to adults and children, and proposes future direction for steps
toward optimal treatment of migraine in patients in France. METHODS: The
recommendations were categorized into 3 levels of proof (A-C) according to
the National Agency for Accreditation and Evaluation in Health (ANAES)
methodology and were based on a professional consensus reached among members
of the Working Group and the Guidelines Review Group of the ANAES. RESULTS:
The International Headache Society diagnostic criteria for migraine should be
used in routine clinical practice. Recommended agents for the treatment of
migraine in adults include nonsteroidal anti-inflammatory drugs,
acetylsalicylic acid (ASA) monotherapy or in combination with metoclopramide,
acetaminophen monotherapy, triptans, ergotamine tartrate, and
dihydroergotamine mesylate. Patients should use the medication as early as
possible after the onset of migraine headache. For migraine prophylaxis in
adults, the following can be used: propranolol, metoprolol, oxetorone, or
amitriptyline as first-line treatment, and pizotifen, flunarizine, valproate
sodium, or topiramate as second-line treatment. Migraine in children can be
distinguished from that in adults by shorter duration (2-48 hours in children
aged <15 years), more frequent bilateral localization, frequent
predominant gastrointestinal disturbances, and frequent pallor hailing the
onset of the attack. The following drugs are recommended in children and
adolescents: ibuprofen in children aged >6 months, diclofenac in children
weighing >16 kg, naproxen in children aged >6 years or weighing >25
kg, ASA alone or in combination with metoclopramide, acetaminophen alone or
in combination with metoclopramide, and ergotamine tartrate in children aged
>10 years. CONCLUSIONS: These guidelines are intended to help general
practitioners to manage migraine patients according to the rules of
evidence-based medicine
|
|
| |
| 11) Treatment guidelines for preventive treatment of migraine. Treatment Guideline Subcommittee of the Taiwan Headache Society.Acta Neurol Taiwan 2008;17(2):132-148. |
文献(ABフォーム)ID
|
11
|
文献PubMed−ID
|
PM: 18686655
|
文献タイトル(日本語)
|
片頭痛予防治療のための治療ガイドライン
|
文献タイトル(英語)
|
Treatment guidelines
for preventive treatment of migraine
|
エビデンスレベル
|
N/A
|
著者名
|
Treatment Guideline Subcommittee of the Taiwan
Headache Society.
|
雑誌名,出版年 巻: 頁
|
Acta Neurol Taiwan.
2008 Jun;17(2):132-48
|
目的
|
エビデンスに基づく台湾での片頭痛の予防治療のために,現在使われる薬剤を評価した.西欧諸国によって提案された治療ガイドラインを参照し,臨床試験の質を評価した.
|
研究デザイン
|
EBM+小委員会メンバーのコンセンサス形成(パネルディスカッション)
|
研究施設
|
台湾頭痛学会
|
研究期間
|
N/A
|
対象患者
|
N/A
|
介入
|
N/A
|
主要評価項目とそれに用いた統計学的手法
|
N/A
|
結果
|
台湾で現在利用可能な片頭痛予防薬物は,β-遮断薬,抗うつ薬,カルシウム拮抗薬,抗てんかん薬,非ステロイド性抗炎症薬,ボツリヌス毒素A型と種々の薬物に分類されることができる.
プロプラノロールは,エビデンスレベルが最も高く,片頭痛予防の第一選択として推奨される.
バルプロ酸,トピラマート,フルナリジンとアミトリプチリンは,第二選択薬として推奨される.
上記の薬物が無効なとき,抗不安薬が使われる.
ボツリヌス毒素A型はエピソード片頭痛予防にならなかったが,慢性片頭痛の有効性はまだ確立されていない.
妊娠中に片頭痛予防薬を使用するのは勧められない.
月経のある女性の片頭痛では,非ステロイド性抗炎症薬とトリプタンが,月経期間に予防的に使われることは可能.
小児や高齢者集団の片頭痛予防薬のエビデンスレベルは,低い.
予防薬は,有効量に投薬する原則は「低用量で開始し,ゆっくり」.
こうすることで有害事象を予防と忍容性を高めることができる.
予防薬の効果判定は,治療後3〜4週まで評価することができない.
片頭痛の改善が4〜6ヵ月間維持した場合,医師は薬を漸減か中止することができる.
医師は,片頭痛予防治療の間,急性頓挫薬を濫用しないように,患者に通知しなければならない.
|
結論
|
N/A
|
作成者
|
渡邉由佳/五十嵐久佳
|
コメント-1
|
ガイドラインは中国語で書かれている.
|
コメント-2
|
|
備考1
|
|
備考2
|
|
備考3
|
|
|
|
論文抄録
|
The
Treatment Guideline Subcommittee of the Taiwan Headache Society evaluated the
medications currently used for preventive therapy of migraine in Taiwan
according to the principles of evidence-based medicine. We assessed the
quality of clinical trials, levels of evidence, and referred to other
treatment guidelines proposed by Western countries. Throughout several panel
discussions, we merged opinions from the subcommittee members in order to
propose a Taiwan consensus about the major roles, recommended levels,
clinical efficacy, adverse events and cautions of clinical practice for these
medications in preventive treatment of migraine. Migraine preventive
medications currently available in Taiwan can be categorized into s-blockers,
antidepressants, calcium channel blockers, anticonvulsants, nonsteroid
anti-inflammatory drugs, botulinum toxin type A and miscellaneous
medications. Propranolol has the best level of evidence, and is recommended
as the first-line medication for migraine prevention. Valproic acid,
topiramate, flunarizine and amitriptyline are suggested as the second-line
medications. The rest medications are used when the above medications fail.
Botulinum toxin type A did not differ from placebo for episodic migraine
prevention but its efficacy in chronic migraine is not determined yet. It is
not recommended to use migraine preventive medication during pregnancy. For
those women with menstrual migraine, nonsteroid anti-inflammatory drug and
triptans can be used for prevention during the menstrual period. The levels
of evidence for migraine preventive medications in children/adolescents and
elderly population are low. The preventive medications should follow the
"start low and go slow" doctrine to reach an effective dosage. This
can prevent adverse events and increase tolerance. The efficacy of preventive
medications can not be evaluated until 3 to 4 weeks after treatment. If the
improvement of migraine maintains for 4 to 6 months, physicians can gradually
taper down or off the medications. Physicians should notify the patients not
to overuse acute medications during migraine prevention treatment.
|
|
| |
| 12) Evers S, Afra J, Frese A, Goadsby PJ, Linde M, May A, Sandor PS; European Federation of Neurological Societies. EFNS guideline on the drug treatment of migraine--revised report of an EFNS task force.2009; Eur J Neurol. 2009; 16(9):968-981. |
文献(ABフォーム)ID
|
12
|
文献PubMed−ID
|
PMID:
19708964
|
文献タイトル(日本語)
|
片頭痛の薬物療法に関するEFNSガイドライン−改訂版
|
文献タイトル(英語)
|
EFNS guideline on the drug treatment of migraine--revised report of an
EFNS task force.
|
エビデンスレベル
|
|
著者名
|
Evers S, Afra J, Frese A, Goadsby PJ, Linde M, May A, Sándor PS;
European Federation of Neurological Societies.
|
雑誌名,出版年 巻: 頁
|
Eur J Neurol. 2009 Sep;16(9):968-81.
|
目的
|
文献検索と専門家委員会のコンセンサスに基づく,片頭痛の薬物療法の根拠に基づく専門家への推奨をすること.
|
研究デザイン
|
N/A
|
研究施設(セッティング)
|
N/A
|
研究期間
|
N/A
|
対象患者,サンプル数
|
N/A
|
介入
|
N/A
|
主要評価項目とそれに用いた統計学的手法
|
N/A
|
結果
|
推奨:
{片頭痛発作の急性治療}
・経口NSAIDとトリプタン
・NSAIDとトリプタンの摂取量の前に,経口メトクロプラミドまたはドンペリドン
・非常に重篤な発作において,静脈内アセチルサリチル酸または皮下スマトリプタンは,第一選択薬
・永続的に使うのはよくないが,cortoicosteroidsまたはジヒドロエルゴタミンも可能
{片頭痛の予防}
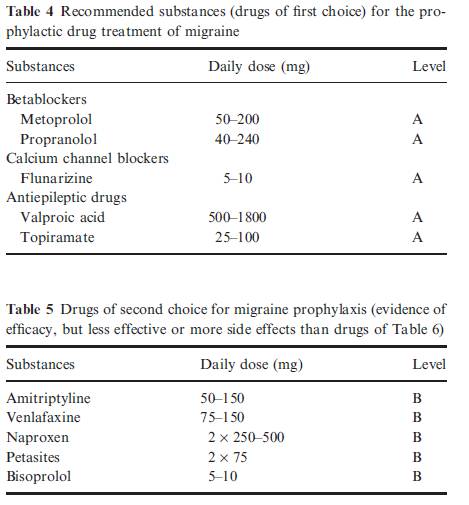
betablockers(プロプラノロールとメトプロロール),フルナリジン,バルプロ酸とトピラマートは,第一選択薬である.
第2選択薬は,アミトリプチリン,ナプロキセン,ペタサイトとビソプロロール
どのような症例に予防薬を使うか
・仕事の任務や学校の日常生活が高度に損なわれるとき.
・月当たりの発作の回数は2回以上である
・片頭痛発作は急性薬物療法に反応しないのが多い場合,非常に長い場合,不快な前兆の時.
・月当たりの片頭痛発作の頻度が3ヵ月以内に少なくとも50%減少する場合,片頭痛予防は成功と考えられる.
・治療評価のために,片頭痛ダイアリーは,有効.
第一選択の薬は,表4で示す.
第一選択薬が有効でない場合,禁忌のとき,または,患者の共存症が表5の薬に関連あるとき,第2または第3選択として推奨される
|
結論
|
|
作成者
|
渡邉由佳/五十嵐久佳
|
コメント-1
|
|
コメント-2
|
|
備考1
|
Migraine
is one of the most frequent disabling neurological conditions with a major
impact on the patients' quality of life. To give evidence-based or expert
recommendations for the different drug treatment procedures of the different
migraine syndromes based on a literature search and an consensus in an expert
panel. All available medical reference systems were screened for all kinds of
clinical studies on migraine with and without aura and on migraine-like
syndromes. The findings in these studies were evaluated according to the
recommendations of the EFNS resulting in level A,B, or C recommendations and
good practice points. For the acute treatment of migraine attacks, oral
non-steroidal anti-inflammatory drugs (NSAIDs) and triptans are recommended.
The administration should follow the concept of stratified treatment. Before
intake of NSAIDs and triptans, oral metoclopramide or domperidon is
recommended. In very severe attacks, intravenous acetylsalicylic acid or
subcutaneous sumatriptan are drugs of first choice. A status migrainosus can
probably be treated by steroids. For the prophylaxis of migraine,
betablockers (propranolol and metoprolol), flunarizine, valproic acid, and
topiramate are drugs of first choice. Drugs of second choice for migraine
prophylaxis are amitriptyline, naproxen, petasites, and bisoprolol.
|
備考2
|
|
備考3
|
|
|
| |
| 13) Bidabadi E, Mashouf M. A randomized trial of propranolol versus sodium valproate for the prophylaxis of migraine in pediatric patients. /Paediatr.Drugs. 2010; 12(4):269-275. |
文献(ABフォーム)ID
|
13
|
文献PubMed−ID
|
PMID: 20593910
|
文献タイトル(日本語)
|
小児片頭痛患者におけるプロプラノロールとバルプロ酸ナトリウムの予防効果無作為比較試験
|
文献タイトル(英語)
|
A randomized trial of propranolol
versus sodium
valproate for the prophylaxis of
migraine in pediatric patients.
|
エビデンスレベル
|
Ib
|
著者名
|
Bidabadi E, Mashouf M
|
雑誌名,出版年 巻: 頁
|
Paediatr.Drugs. 2010; 12(4):269-275.
|
目的
|
小児片頭痛患者におけるプロプラノロールおよびバルプロ酸ナトリウムの片頭痛予防効果の比較
|
研究デザイン
|
無作為比較試験
|
研究施設
|
|
研究期間
|
6カ月の予防療法期間
|
対象患者
|
小児片頭痛患者(n=63, 5-15歳)
|
介入
|
Group A(32人)はプロプラノロール(3mg/kg/日)
Group B(31人)はバルプロ酸ナトリウム(30mg/kg/日) を内服.
|
主要評価項目とそれに用いた統計学的手法
|
|
結果
|
頭痛頻度は,プロプラノロール投与患者の83%でベースラインから50%以上減少し,バルプロ酸ナトリウム投与患者では63%が減少した.1カ月あたりの平均頭痛頻度は,プロプラノロール群で13.8回から4.2回に減少し,バルプロ酸群では13.2回から5.8回 に減少した.頭痛の持続時間も両群で減少した.
|
結論
|
小児の前兆のない片頭痛の予防にプロプラノロールおよびバルプロ酸ナトリウムの有効性を示した.
|
作成者
|
島津智一/荒木信夫/竹島多賀夫
|
コメント-1
|
|
コメント-2
|
|
備考1
|
Publication Types
·
Comparative Study
·
Randomized Controlled Trial
MeSH Terms
·
Adolescent
·
Child
·
Child, Preschool
·
Humans
·
Migraine
Disorders/prevention & control*
·
Propranolol/pharmacology*
·
Time Factors
·
Valproic Acid/pharmacology*
Substances
·
Propranolol
·
Valproic Acid
|
備考2
|
|
備考3
|
|
備考4
|
|
論文抄録
|
BACKGROUND:
Migraine is the most common of the paroxysmal disorders to affect the brain in the pediatric population. Both propranolol andsodium
valproate (valproic acid) have been advocated as prophylactic
agents for childhood migraine.
OBJECTIVE:
To compare the efficacy and tolerability of propranolol and sodium
valproate in the prevention of migraine in
the pediatric population.
METHODS:
Sixty-three children (aged 5-15 years) with migraine without aura, as defined by the 2004
International Headache Society (IHS) criteria, were included in this
prospective, double-blind clinical trial and
were randomly assigned to two groups. Group A (n = 32 patients)
received propranolol3
mg/kg/day and group B (n = 31 patients) received sodium valproate 30
mg/kg/day, with at least 6 months of follow up. The propranolol dosage was adjusted to 2 mg/kg/day
and the sodium
valproate dosage to 15
mg/kg/day, after the first follow-up visit. Participants were evaluated by
using a detailed questionnaire that asked about the features of headaches and
general health characteristics. The study endpoints were successful treatment
for a 4- to 6-month period; 3 months of a persistent unsuccessful or
incomplete response to treatment; intolerable side effects; and/or patient
non-adherence. All data were analyzed longitudinally by comparing baseline
data with data from each follow-up.
RESULTS:
A total of 60 patients completed
the full headache prophylaxis period.
The baseline headache frequency was reduced by more than 50% in 83% of propranolol recipients and in 63% of sodium
valproate recipients
(statistically not significant); the overall reduction of baseline headache
frequency per month was better in group A (p = 0.044). The mean headache
frequency per month was reduced from 13.86 +/- 2.11 to 4.23 +/- 3.24 in group
A, and from 13.23 +/- 2.43 to 5.83 +/- 4.04 in group B; the difference
between the two groups was statistically significant (p < 0.01). The mean
headache duration per week was decreased from 9.9 +/- 7.4 hours to 3.2 +/-
5.9 hours in group A, and from 9.1 +/- 6.9 hours to 3.7 +/- 5.0 hours in
group B; although there was no statistically significant difference between propranolol and sodium
valproate, headache duration was markedly improved with each drug (p
< 0.002). Reduction of headache severity by at least one grade was seen in
64% of patients in group A and in 56% in group B,
and complete cessation of headache attacks occurred in 14% of patients in group A and 10% in group B (not
significant). Minor side effects appeared to be fairly well tolerated by patients in both groups, with no significant
difference in side effects between the two groups.
CONCLUSION:
This prospective study supports the efficacy of propranolol and sodium
valproate as prophylaxis for pediatric migraine without aura, based on IHS criteria.
There were no significant differences between these two drugs in all
evaluated parameters except for the mean headache frequency per month, which
was lower with propranolol than
with sodium
valproate.
|
|