| 1) Ayata C, Jin H, Kudo C, Dalkara T, Moskowitz MA: Suppression of cortical spreading depression in migraine prophylaxis. Ann Neurol. 2006; 59(4): 652-661. |
文献(ABフォーム)ID
|
1
|
文献PubMed-ID
|
PMID: 16450381
|
文献タイトル(日本語)
|
片頭痛予防薬のCSDの抑制
|
文献タイトル(英語)
|
Suppression of cortical
spreading depression in migraine prophylaxis.
|
エビデンスレベル
|
IIb
|
著者名
|
Ayata C, Jin H, Kudo C, Dalkara T, Moskowitz MA.
|
雑誌名,出版年 巻: 頁
|
Ann Neurol 2006; 59(4): 652-661.
|
目的
|
Topiramate,
valproate, propranolol, amitriptyline, and methysergide have been widely
prescribed for migraine prophylaxis, but their mechanism or site of action is
uncertain. Cortical spreading depression (CSD) has been implicated in
migraine and as a headache trigger and can be evoked in experimental animals
by electrical or chemical stimulation. We hypothesized that migraine
prophylactic agents suppress CSD as a common mechanism of action.
|
研究デザイン
|
|
研究施設
|
|
研究期間
|
|
対象患者
|
|
介入
|
Rats were treated either acutely or
chronically over weeks and months, with one of the above migraine prophylactic drugs, vehicle, or
D-propranolol, a clinically ineffective drug. The impact of treatment was
determined on the frequency of evoked CSDs after topical potassium
application or on the incremental cathodal stimulation threshold to evoke
CSD.
|
主要評価項目とそれに用いた統計学的手法
|
The electrophysiological and systemic
physiological data and the number of CSDs after topical KCl were statistically
analyzed using Student’s t test or one-way analysis of variance
followed by Dunnett’s multiple comparisons test versus control group.
|
結果
|
Chronic daily
administration of migraine prophylactic drugs dose-dependently suppressed CSD
frequency by 40 to 80% and increased the cathodal stimulation threshold,
whereas acute treatment was ineffective. Longer treatment durations produced
stronger CSD suppression. Chronic D-propranolol treatment did not differ from
saline control.
|
結論
|
Our data
suggest that CSD provides a common therapeutic target for widely prescribed
migraine prophylactic drugs. Assessing CSD threshold may prove useful for
developing new prophylactic drugs and improving upon existing ones.
|
作成者
|
菊井祥二/竹島多賀夫
|
コメント-1
|
プロプラノロールの片頭痛予防作用は末梢血管や自律神経へのβ遮断作用ばかりでなく,中枢における神経伝達に関与する可能性も示唆される.
|
コメント-2
|
|
備考1
|
|
備考2
|
|
備考3
|
|
論文抄録
|
OBJECTIVE: Topiramate,
valproate, propranolol, amitriptyline, and methysergide have been widely
prescribed for migraine prophylaxis,
but their mechanism or site of action is uncertain. Cortical
spreading depression (CSD) has been implicated in migraine and as a headache trigger and can be evoked
in experimental animals by electrical or chemical stimulation. We
hypothesized that migraine prophylactic agents
suppress CSD as a common mechanism of action.
METHODS: Rats were treated
either acutely or chronically over weeks and months, with one of the above migraine prophylactic drugs, vehicle, or
D-propranolol, a clinically ineffective drug. The impact of treatment was
determined on the frequency of evoked CSDs after topical potassium
application or on the incremental cathodal stimulation threshold to evoke
CSD.
RESULTS: Chronic daily
administration of migraine prophylactic drugs
dose-dependently suppressed CSD frequency by 40 to 80% and increased the
cathodal stimulation threshold, whereas acute treatment was ineffective.
Longer treatment durations produced stronger CSD suppression.
Chronic D-propranolol treatment did not differ from saline control.
INTERPRETATION: Our data
suggest that CSD provides a common therapeutic target for widely prescribed migraine prophylactic drugs. Assessing CSD threshold
may prove useful for developing new prophylactic drugs and improving upon
existing ones.
|
|
| |
| Holroyd KA, Penzien DB, Cordingley GE: Propranolol in the management of recurrent migraine: a meta-analytic review. Headache 1991; 31(5): 333-340. |
文献(ABフォーム)ID
|
2
|
文献PubMed-ID
|
PMID:1830566
|
文献タイトル(日本語)
|
再発性片頭痛管理におけるプロプラノロール:メタ解析レビュー
|
文献タイトル(英語)
|
Propranolol in the management of recurrent migraine: a
meta-analytic review.
|
エビデンスレベル
|
Ia
|
著者名
|
Holroyd,K.A.; Penzien,D.B.; Cordingley,G.E.
|
雑誌名,出版年 巻: 頁
|
Headache. 1991; 31(5): 333-340
|
目的
|
β遮断薬プロプラノロールの片頭痛予防療法を評価した研究から有効性を検索する.
|
研究デザイン
|
Meta-analysis
|
研究施設
|
|
研究期間
|
|
対象患者
|
53の臨床試験(プロプラノロールで治療された片頭痛患者2403人)
|
介入
|
Medlineなどの医学文献分析検索システム・データベースで成人片頭痛患者でプロプラノロールで治療された5症例以上の報告,片頭痛改善の度合いを表したものがあるものをコンピューター検索した.
|
主要評価項目とそれに用いた統計学的手法
|
頭痛治療インデックス(H.I.)を治療前vsプロプラノロール,プロプラノロールvsプラセボ,プラセボvsプロプラノロールで算出した.
|
結果
|
プロプラノロール典型的な投与量は160mg/日であった.
二重盲検試験でのプロプラノロール有効率は平均43.7%で,プラセボの有効率14.3%より有意に高値(p<0.001)であった.
頭痛日記を用いた評価ではプロプラノロールは片頭痛発作を44%減少させた.古典的な患者の自覚的改善度や臨床的な有効性で評価するとプロプラノロールは片頭痛を65%改善させた.プラセボではいずれの評価法でも約14%の片頭痛改善を認めた.
研究により投与量が異なっているが,投与量と片頭痛予防効果の用量-反応関係は明確ではなかった.
プロプラノロールの認容性は良好であった.
|
結論
|
β遮断薬プロプラノロールの片頭痛予防薬としての効果は確実である
|
作成者
|
井尻珠美/竹島多賀夫
|
コメント-1
|
研究およびレポートの質は高い.ただし,解析対象の研究報告は古いものが多く現在の基準からは不完全な臨床試験を対象としたメタアナリシスである.
|
コメント-2
|
|
備考1
|
Publication
Types:
- Clinical Trial
- Meta-Analysis
MeSH Terms:
- Adult
- Female
- Human
- Male
- Meta-Analysis
- Migraine/drug
therapy*
- Migraine/physiopathology
- Migraine/prevention
& control
- Prognosis
- Propranolol/adverse
effects
- Propranolol/therapeutic
use*
- Recurrence
Substances:
|
備考2
|
hed_3105333.pdf
|
備考3
|
|
備考4
|
|
論文抄録
|
We
used meta-analytic statistical techniques to synthesize findings from studies
that evaluated propranolol HCI for the prevention of recurrent migraine
(2,403 treated patients). The modal migraine sufferer treated in these
studies was a female, about 37 years of age, who suffered from common (rather
than classical) migraines and reported a 17-year history of problem
migraines. The modal treatment was 160 mg. propranolol per day. Meta-analysis
revealed that, on average, propranolol yielded a 44% reduction in migraine
activity when daily headache recordings were used to assess treatment
outcome, and a 65% reduction in migraine activity when less conservative
measures (e.g., clinical ratings of improvement, global patient reports) were
used. Meta-analysis thus revealed substantial support for short-term
effectiveness of propranolol. However, little information was available
concerning the long-term effectiveness of propranolol.
|
|
| |
| Kangasniemi P, Andersen AR, Andersson PG, Gilhus NE, Hedman C, Hultgren M, Vilming S, Olesen J: Classic migraine: effective prophylaxis with metoprolol. Cephalalgia 1987; 7(4): 231-238. |
文献(ABフォーム)ID
|
3
|
文献PubMed-ID
|
PMID:
3322569
|
文献タイトル(日本語)
|
古典的片頭痛:メトプロロールによる予防効果
|
文献タイトル(英語)
|
Classic migraine: effective prophylaxis
with metoprolol.
|
エビデンスレベル
|
Ib
|
著者名
|
Kangasniemi P, Andersen AR,
Andersson PG et al.
|
雑誌名,出版年 巻: 頁
|
Cephalalgia. 1987; 7: 231-238
|
目的
|
β遮断薬メトプロロールの古典的片頭痛予防効果を確認する
|
研究デザイン
|
二重盲検交差試験(a double-blind cross-over study)
|
研究施設
|
スカンジナビアの神経センター8施設
|
研究期間
|
1984年10月から1985年12月
|
対象患者
|
1ヶ月に2-8回の発作がある16歳~65歳の古典的片頭痛患者 77例
73例が試験を完了
前兆を伴う発作1119回,前兆を伴わない発作374回が記録された.
|
介入
|
導入期(run-in period): 4w
washout: 4w
メトプロロール徐放錠(Durules 200mg)を1日1回(朝)に内服し,偽薬と比較: 8w
|
主要評価項目とそれに用いた統計学的手法
|
発作頻度,平均発作持続時間,全般評価,発作あたりの鎮痛薬の使用量
|
結果
|
メトプロロールは,発作頻度(1.8対2.5発作/4週),平均発作持続時間(6.0hr 対 8.0h/発作),平均の全般評価,発作あたりの鎮痛薬の使用量は偽薬よりすぐれていた.
|
結論
|
メトプロロールは古典的片頭痛の予防に有効である.
|
作成者
|
竹島多賀夫
|
コメント-1
|
中規模の多施設RCTで良質な研究.
|
コメント-2
|
|
備考1
|
Publication
Types:
- Clinical Trial
- Controlled
Clinical Trial
MeSH Terms:
- Adolescent
- Adult
- Clinical Trials
- Delayed-Action
Preparations
- Double-Blind
Method
- Female
- Humans
- Male
- Metoprolol/administration
& dosage
- Metoprolol/adverse
effects
- Metoprolol/therapeutic
use*
- Middle Aged
- Migraine/prevention
& control*
- Random
Allocation
Substances:
- Delayed-Action
Preparations
- Metoprolol
|
備考2
|
|
備考3
|
|
備考4
|
|
論文抄録
|
Metoprolol slow-release tablets (Durules), 200 mg,
given once daily in the morning were compared
with placebo in the prophylaxis of classic migraine.
The trial comprised eight Scandinavian neurologic
centres and was designed as a double-blind cross-over
study with 4 weeks' run-in, four weeks washout, and
8 weeks of either treatment. Seventy-seven patients
with two to eight migraine attacks per month were
entered in the trial, and 73 completed it. A total of 1119
attacks with aura symptoms and 374 without were recorded.
Metoprolol was significantly better than placebo with regard to
the total frequency of attacks (1.8 versus 2.5 attacks/4 weeks),
mean duration of attacks (6.0 versus 8.0 h/attack),
mean global rating, and consumption of analgesics per attack.
Similar differences could be shown for attacks
with aura symptoms alone,
except for the duration of attacks. Metoprolol is the
first drug for which a prophylactic effect
in classic migraine has been convincingly demonstrated |
|
| |
| Steiner TJ, Joseph R, Hedman C, Rose FC: Metoprolol in the prophylaxis of migraine: parallel-groups comparison with placebo and dose-ranging follow-up. Headache 1988; 28(1): 15-23. |
文献(ABフォーム)ID
|
4
|
文献PubMed-ID
|
PMID:
32771636
|
文献タイトル(日本語)
|
メトプロロールによる片頭痛予防療法:プラセボとの比較と容量依存性
の追跡
|
文献タイトル(英語)
|
Metoprolol in the prophylaxis of migraine: parallel-groups
comparison with placebo and dose-ranging follow-up.
|
エビデンスレベル
|
Ib
|
著者名
|
Steiner TJ, Joseph R, Hedman C et al.
|
雑誌名,出版年 巻: 頁
|
Headache. 1988; 28:15-23
|
目的
|
β遮断薬メトプロロールが容量依存的に片頭痛の発作回数・程度を抑制可能か否かを検討
|
研究デザイン
|
二重盲検プラセボ対照試験(a double-blind placebo-controlled trial)
|
研究施設
|
The Princess Margaret Clinic for treatment of migraine
|
研究期間
|
|
対象患者
|
少なくとも2年の罹病期間がある古典型片頭痛,普通型片頭痛患者で,予防療法が必要な18歳~64歳までの88例.
|
介入
|
1ヶ月のプラセボによる観察期間の後,治療不要となった29症例を除外 (Baseline period).
59例はランダムに50mg×2回/日の偽薬またはメトプロロールを2ヶ月間投与 (Double-blind period).
治療効果が不十分な場合には,盲検下に偽薬はメトプロロール50mg×2回に増量,メトプロロール50mg×2回は100mg×2回に増量し,最高3ヵ月の追跡調査期間を設定 (Follow-up period).
|
主要評価項目とそれに用いた統計学的手法
|
頭痛日記に片頭痛発作の有無, 片頭痛発作の重症度,急性期治療薬の使用数を記録
|
結果
|
最初の1ヶ月間でのプラセボ効果は40%に認められた.
Double-blind periodにおいてメトプロロールは偽薬より有意に発作頻度を減少させたが,頭痛発作の重症度は治療により変化しなかった.
Follow-up periodに偽薬治療からメトプロロールに切り替えた患者にも改善がみられ,高用量のメトプロロール変更群も統計学的に有意なさらなる改善がみられた.
副作用は軽度で可逆性であった.
|
結論
|
メトプロロールには片頭痛発作予防効果がある.
患者毎に用量設定をすることで実質的な有効性を強化することができる.
副作用は問題にならず,片頭痛治療において選択的β1遮断薬が,非選択的β遮断薬より好まれる可能性が示唆された.
|
作成者
|
竹島多賀夫
|
コメント-1
|
中規模の良質なRCT.
|
コメント-2
|
|
備考1
|
Publication
Types:
- Clinical Trial
- Controlled
Clinical Trial
MeSH Terms:
- Adult
- Clinical Trials
- Dose-Response
Relationship, Drug
- Double-Blind
Method
- Female
- Follow-Up
Studies
- Humans
- Male
- Metoprolol/administration
& dosage*
- Middle Aged
- Migraine/prevention
& control*
- Research
Support, Non-U.S. Gov't
Substances:
|
備考2
|
|
備考3
|
|
論文抄録
|
88
patients in need of prophylactic treatment for classical, common or mixed
migraine of at least 2 years' duration were admitted to a double-blind
placebo-controlled trial of the beta1-selective adrenoceptor blocker,
metoprolol. All patients initially took placebo for I month, during which 29
were excluded principally because of failure to reattend or placebo-response
making active treatment unnecessary. The remaining 59 patients were
randomised to continued placebo or metoprolol 50 mg b.i.d. for 2 months. Patients
after this time subjectively categorizing their responses as less than
optimal changed, double-blindly,
from placebo to metoprolol 50 mg b.i.d., or from metoprolol 50 mg b.i.d. to
100 mg b.i.d., for a further follow-up period of up to 3 months. Placebo
response was 40% overall, and often occurred after the first month. In the
first double-blind comparative period metoprolol reduced attack frequency
significantly, and more than placebo. Severity of attacks still occurring was
not altered by either treatment. Other measures of illness were altered
consistently with these principal findings. Consistent improvements also were
seen in patients switching from initial placebo therapy to metoprolol 50 mg
b.i.d. for the further follow-up period, and those changing to the higher
dose of metoprolol showed statistically significant further improvements, and
clinically important improvements overall. Side-effects were minor and
reversible. This study gives supportive evidence of the value of metoprolol
in preventing migraine attacks and suggests that individual dosage titration
can substantially enhance its efficacy. Side-effects do not significantly
impede its use and other evidence suggests that beta1-selective blockers are
to be preferred over non-selective in migraine therapy.
|
|
| |
| Stellar S, Ahrens SP, Meibohm AR, Reines SA: Migraine prevention with timolol. A double-blind crossover study. JAMA 1984; 252(18): 2576-2580. |
文献(ABフォーム)ID
|
5
|
文献PubMed-ID
|
PMID: 6387197
|
文献タイトル(日本語)
|
チモロールによる片頭痛予防:二重盲検交差試験
|
文献タイトル(英語)
|
Migraine prevention with timolol. A
double-blind crossover study.
|
エビデンスレベル
|
Ib
|
著者名
|
Stellar S, Ahrens SP, Meibohm AR
et al.
|
雑誌名,出版年 巻: 頁
|
JAMA. 1984; 252:2576-2580
|
目的
|
β遮断薬チモロールが片頭痛予防薬として効果的かどうか決定すること.
|
研究デザイン
|
二重盲検交差試験 (A double-blind crossover study)
|
研究施設
|
|
研究期間
|
|
対象患者
|
18歳~66歳の片頭痛患者107例(女性,77例,男性30例)
|
介入
|
マレイン酸チモロール(20~30mg/日),又は偽薬を予防投与
20週観察,二重盲検交叉試験
|
主要評価項目とそれに用いた統計学的手法
|
1)28日ごとの頭痛頻度
2)頭痛頻度の観察期からの変化率
3)レスポンダー(50%以上の発作減少)の数
4)4,8週の全般改善度
5)患者による全般的評価
6)患者の嗜好
7)頭痛発作の重症度,持続時間,随伴症状
|
結果
|
94例が試験を完了した.
チモロールはレスポンダー(50%以上の発作減少)の数,頭痛頻度,全般改善度,患者の嗜好の項目において,偽薬より有意に改善がみられた.
全般改善度は偽薬40%,チモロール65%であった.
重症度と頭痛発作の持続期間は不変であった.
両群とも副作用はほとんどみられなかった.
|
結論
|
β遮断薬チモロールは発作頻度の高い片頭痛患者の安全かつ有効な治療である.
|
作成者
|
竹島多賀夫
|
コメント-1
|
良質なRCT
|
コメント-2
|
|
備考1
|
Publication
Types:
- Clinical Trial
- Randomized
Controlled Trial
MeSH Terms:
- Adolescent
- Adult
- Aged
- Clinical Trials
- Double-Blind
Method
- Female
- Humans
- Male
- Middle Aged
- Migraine/prevention
& control*
- Random
Allocation
- Timolol/administration
& dosage
- Timolol/adverse
effects
- Timolol/therapeutic
use*
Substances:
|
備考2
|
|
備考3
|
|
備考4
|
|
論文抄録
|
One hundred seven patients (77 women and 30 men) with
migraine headache were given prophylactic treatment with timolol maleate,
20 to 30 mg/day, or matching placebo during a 20-week,
double-blind crossover study. Among the 94 patients
who completed the study, timolol was significantly better than
placebo in terms of decrease in frequency of headaches from baseline,
numbers of patients who had a 50%
reduction in headache frequency, global response, and patient preference.
Overall global response rates were 65% with timolol compared with 40%
with placebo. The severity and duration of headaches
that occurred were unchanged.
Few side effects were reported with either timolol or placebo.
The study demonstrates that the beta-blocker timolol is a safe
and effective treatment in patients with frequent migraine headaches. |
|
| |
| Johannsson V, Nilsson LR, Widelius T, Javerfalk T, Hellman P, Akesson JA, Olerud B, Gustafsson CL, Raak A, Sandahl G, et al: Atenolol in migraine prophylaxis a double-blind cross-over multicentre study. Headache 1987; 27(7): 372-374. |
文献(ABフォーム)ID
|
6
|
文献PubMed-ID
|
PMID: 3308768
|
文献タイトル(日本語)
|
アテノロールによる片頭痛予防 多施設二重盲検交叉試験
|
文献タイトル(英語)
|
Atenolol in
migraine prophylaxis a double-blind cross-over multicentre study.
|
エビデンスレベル
|
Ib
|
著者名
|
Johannsson V, Nilsson LR, Widelius T et al.
|
雑誌名,出版年
巻: 頁
|
Headache.
1987; 27(7): 372-374
|
目的
|
アテノロールの片頭痛予防効果を検討する.
|
研究デザイン
|
多施設二重盲検交叉試験 (a double-blind cross-over multicentre study)
|
研究施設
|
12施設
|
研究期間
|
|
対象患者
|
少なくとも月に2回発作のある古典型片頭痛または普通型片頭痛に罹患している63例
|
介入
|
Period 1(Wash-out/run-in period):8w
Period 2,4:アテノロール100mg,または偽薬を24w投与
Period 3(Wash-out period):2w
|
主要評価項目とそれに用いた統計学的手法
|
頭痛インデックス(片頭痛発作の頻度,程度,随伴症状を含む)
|
結果
|
アテノロール群は,頭痛インデックスが70%改善(p = 0.004)し,頭痛日数〔率〕が59%の患者(p = 0.010)で減少した.
副作用はほとんどなかった.
|
結論
|
アテノロールは安全かつ有効な片頭痛予防薬である.
|
作成者
|
竹島多賀夫
|
コメント-1
|
RCT.データの詳細は公表(記載)されていないので,信頼性に関する評価は困難である.
|
コメント-2
|
|
備考1
|
Publication Types:
- Clinical Trial
- Controlled Clinical Trial
MeSH Terms:
- Adult
- Atenolol/adverse effects
- Atenolol/therapeutic use*
- Clinical Trials
- Double-Blind Method
- Female
- Humans
- Male
- Middle Aged
- Migraine/prevention & control*
Substances:
|
備考2
|
|
備考3
|
|
備考4
|
|
論文抄録
|
The prophylactic
anti-migraine effect of atenolol was compared to placebo in a multicentre
study on 63 patients with classical and/or common migraine. The study design
was double-blind cross-over and patients were given atenolol 100 mg o.d. or
matching placebo during a study treatment period of 24 weeks. The effect of
atenolol was significantly better than that of placebo: integrated headache
values were reduced in 70% of the patients (p = 0.004) and the proportion of
days with headache was reduced in 59% of the patients (p = 0.010). Few side effects
were reported with both atenolol and placebo. This study shows atenolol to be safe and effective in the prophylactic treatment of migraine.
|
|
| |
| Ryan RE Sr: Comparative study of nadolol and propranolol in prophylactic treatment of migraine. Am Heart J 1984; 108 (4 Pt 2): 1156-1159. |
文献(ABフォーム)ID
|
7
|
文献PubMed-ID
|
PMID: 6148878
|
文献タイトル(日本語)
|
片頭痛予防療法におけるナドロールとプロプラノロール比較試験
|
文献タイトル(英語)
|
Comparative study of nadolol and propranolol in
prophylactic treatment of migraine.
|
エビデンスレベル
|
Ib
|
著者名
|
Ryan RE Sr.
|
雑誌名,出版年 巻: 頁
|
Am. Heart J. 1984; 108: 1156-1159.
|
目的
|
β遮断薬ナドロールとプロプラノロールのどちらが片頭痛予防薬として効果的かどうか決定する.
|
研究デザイン
|
無作為二重盲検試験(double-blind
randomized study)
|
研究施設
|
Ryan Headache Center
|
研究期間
|
|
対象患者
|
月に3回以上の発作をおこしている21歳~60歳の片頭痛患者48人.
|
介入
|
Period A: placebo 4w
引き続き Period
B: 12w
Group A(16人)はナドロール80mg/day,Group B(16人)はナドロール160mg/day,Group C(16人)はプロプラノロール160mg/dayを内服.
|
主要評価項目とそれに用いた統計学的手法
|
プライマリーエンドポイントは頭痛の頻度と程度.
日記に頭痛の重症度,頭痛時間,頓挫薬服用量,頭痛の前駆症状,月経期間などの付随事項,副作用などを記入.
|
結果
|
ナドロール80mg群では頭痛回数が6.13回/月から2.74回/月,ナドロール160mg群では5.56回/月から2.93回/月,プロプラノロール群では7.42回/月から4.54回/月と全ての群で改善がみられた.最も頻度が減少したのはナドロール80mg群であった.
48人中ナドロール80mg群の患者が一人だけが副作用により脱落し,副作用は少ないと考えられた.
|
結論
|
3群とも片頭痛予防薬として有効であったが,最も有効だったものはナドロール80mgであった群.ナドロール80mgはプロプラノロール160mgよりも有効と考えられた.
|
作成者
|
井尻珠美/竹島多賀夫
|
コメント-1
|
よくデザインされたRCT.
いつくかの追試が必要.
|
コメント-2
|
|
備考1
|
Publication
Types:
- Clinical Trial
- Randomized
Controlled Trial
MeSH Terms:
- Adrenergic
beta-Antagonists/therapeutic use*
- Adult
- Clinical Trials
- Comparative
Study
- Double-Blind
Method
- Female
- Human
- Male
- Middle Aged
- Migraine/prevention
& control*
- Nadolol
- Propanolamines/therapeutic
use*
- Propranolol/therapeutic
use*
- Random
Allocation
Substances:
- Adrenergic
beta-Antagonists
- Propanolamines
- Nadolol
- Propranolol
|
備考2
|
|
備考3
|
|
論文抄録
|
Forty-eight
patients (13 men and 35 women) took part in a double-blind randomized study.
All patients received a placebo daily for 4 weeks (period A), at the end of
which the frequency and severity of headaches experienced by each patient
were assessed. Patients then received an active drug for 12 weeks (period B).
Sixteen patients received nadolol, 80 mg/day; 16
received nadolol, 160 mg/day; and 16 received propranolol, 160 mg/day. The frequency and severity of
headaches in the three groups were tabulated at the end of period B, as were
the side effects. Only three subjects dropped out during the study, and one
of these needed abdominal surgery. All three groups reported improvement, the
most noticeable being in those patients who received 80 mg of nadolol daily.
|
|
| |
| Diener HC, Matias-Guiu J, Hartung E, Pfaffenrath V, Ludin HP, Nappi G, De Beukelaar F: Efficacy and tolerability in migraine prophylaxis of flunarizine in reduced doses: a comparison with propranolol 160 mg daily. Cephalalgia 2002; 22(3): 209-221. |
文献(ABフォーム)ID
|
8
|
文献PubMed-ID
|
PMID: 12047461
|
文献タイトル(日本語)
|
片頭痛予防療法における減量でのフルナリジンの効果と忍容性:プロプラノロール160mg/日との比較.
|
文献タイトル(英語)
|
Efficacy and tolerability in migraine prophylaxis of flunarizine in reduced doses: a comparison with propranolol 160 mg daily.
|
エビデンスレベル
|
Ib
|
著者名
|
Diener HC, Matias-Guiu J, Hartung E, Pfaffenrath V, Ludin HP, Nappi G, De Beukelaar F.
|
雑誌名,出版年 巻: 頁
|
Cephalalgia. 2002; 22(3): 209-221.
|
目的
|
To assess the efficacy and tolerability of two doses of flunarizine (10 mg o.d.=FLU 10 mg and 5 mg o.d.=FLU 5 mg) in the prophylaxis of migraine, in comparison with slow-release propranolol (160 mg o.d.).
|
研究デザイン
|
Phase-IV
double-blind equivalence trial
|
研究施設
|
Department of
Neurology, University Essen, Germany.
|
研究期間
|
16週間
|
対象患者
|
808人.
|
介入
|
A total of 808 subjects were treated in
a treatment period of 16 weeks. 142 subjects discontinued the trial
prematurely, mainly because of adverse events (n=58). The mean attack
frequency in the double-blind period was 2.0 for the FLU 5 mg group, 1.9 for
the FLU 10 mg group, and 1.9 for the propranolol group. The mean attack frequency in the last 28 days of the double-blind
period was 1.8 for FLU 5 mg, 1.6 for FLU 10 mg, and 1.7 for propranolol.
|
主要評価項目とそれに用いた統計学的手法
|
|
結果
|
Both flunarizine groups were at least as effective as propranolol (P<0.001 in one-sided test). The
percentage of responders (defined as subjects for whom attack frequency
decreased by at least 50% compared to run-in) in the last 28 days of the
double-blind period was 46% (118/259) for FLU 5 mg, 53% (141/264) for FLU 10
mg, and 48% (125/258) for propranolol.
Statistical analysis showed that FLU 10 mg is at least as effective as propranolol (P<0.001) and showed a trend for
noninferiority of FLU5 and propranolol (P=0.053). No
statistically significant differences between the treatment groups were found
for any of the secondary parameters. Overall, 190 subjects reported one or
more adverse events during the run-in phase: 54 (20.5%) in the FLU 5 mg
group, 76 (27.7%) in the FLU 10 mg group and 60 (22.3%) in the propranolol group.
|
結論
|
10 mg flunarizine daily with a
drug-free weekend is at least as effective as 160 mg propranolol in the prophylaxis of migraine for all evaluated parameters (one-sided
equivalence tests) after 16 weeks of treatment. In addition, 5 mg flunarizine proves to be at least as effective as 160 mg propranolol when
looking at the mean attack frequency for both the whole double-blind period
and the last 28 days of treatment.
|
作成者
|
菊井祥二/竹島多賀夫
|
コメント-1
|
プロプラノロール160mg/日とフルナリジン10mg/日の片頭痛予防効果はほぼ同等である.
|
コメント-2
|
|
備考1
|
|
備考2
|
|
備考3
|
|
論文抄録
|
This was a phase-IV double-blind equivalence trial
designed to assess the efficacy and tolerability of two doses of flunarizine
(10 mg o.d.=FLU 10 mg and 5 mg o.d.=FLU 5 mg) in the prophylaxis of migraine,
in comparison with slow-release propranolol (160 mg o.d.). A total of 808
subjects were treated in a treatment period of 16 weeks. 142 subjects
discontinued the trial prematurely, mainly because of adverse events (n=58).
The mean attack frequency in the double-blind period was 2.0 for the FLU 5 mg
group, 1.9 for the FLU 10 mg group, and 1.9 for the propranolol group. The
mean attack frequency in the last 28 days of the double-blind period was 1.8
for FLU 5 mg, 1.6 for FLU 10 mg, and 1.7 for propranolol. Both flunarizine
groups were at least as effective as propranolol (P<0.001 in one-sided
test). The percentage of responders (defined as subjects for whom attack
frequency decreased by at least 50% compared to run-in) in the last 28 days
of the double-blind period was 46% (118/259) for FLU 5 mg, 53% (141/264) for
FLU 10 mg, and 48% (125/258) for propranolol. Statistical analysis showed
that FLU 10 mg is at least as effective as propranolol (P<0.001) and showed
a trend for noninferiority of FLU5 and propranolol (P=0.053). No
statistically significant differences between the treatment groups were found
for any of the secondary parameters. Overall, 190 subjects reported one or
more adverse events during the run-in phase: 54 (20.5%) in the FLU 5 mg
group, 76 (27.7%) in the FLU 10 mg group and 60 (22.3%) in the propranolol
group. The results of this equivalence trial show that 10 mg flunarizine
daily with a drug-free weekend is at least as effective as 160 mg propranolol
in the prophylaxis of migraine for all evaluated parameters (one-sided
equivalence tests) after 16 weeks of treatment. In addition, 5 mg flunarizine
proves to be at least as effective as 160 mg propranolol when looking at the
mean attack frequency for both the whole double-blind period and the last 28
days of treatment. However, in the analysis of responders, 160 mg propranolol
seems to be slightly better than 5 mg flunarizine. In addition, no
significant differences between the three treatments were found with regard
to safety: all three treatments were generally well-tolerated and safe.
|
|
| |
| Kaniecki RG: A comparison of divalproex with propranolol and placebo for the prophylaxis of migraine without aura. Arch Neurol 1997; 54(9): 1141-1145. |
文献(ABフォーム)ID
|
9
|
文献PubMed-ID
|
PMID: 9311358
|
文献タイトル(日本語)
|
前兆のない片頭痛の予防治療におけるバルプロ酸とプロプラノロールの比較
|
文献タイトル(英語)
|
A comparison of
divalproex with propranolol and placebo for the prophylaxis of migraine
without aura.
|
エビデンスレベル
|
Ib
|
著者名
|
Kaniecki RG.
|
雑誌名,出版年 巻: 頁
|
Arch Neurol. 1997; 54(9): 1141-1145.
|
目的
|
前兆のない片頭痛の予防療法における塩酸プロプラノロール(および,偽薬)とdivalproexナトリウム(Depakote)の有効性を比較する.
|
研究デザイン
|
単一の-研究者による,5種類の治療期間をもつランダム化二重盲検プラセボ対照試験:
ベースライン(週1-4)→偽薬(週5-8)→第1の治療期間(1薬剤,週9-20)→休薬期間(週21-24)→第2の治療期間(他薬剤,週25-36).
|
研究施設
|
頭痛疾患を専門とする一般の神経内科開業医
|
研究期間
|
36週間
|
対象患者
|
37例の片頭痛患者(30人の女性と7人の男性)で,32例が評価対象となった.
|
介入
|
対象患者全員にまずプラセボを使用し,その後半数の患者はバルプロ酸,残りの患者はプロプラノロールを使用した.その後,休薬期間を経て他剤の使用を行った.
バルプロ酸とプロプラノロール服用量は、各12週治療サイクルの最初の8週間で決定した.
バルプロ酸は23名には1500 mg/d,2名には2000mg/dを投与し,7名は2000mg/dを1500 mg/dに下げて投与した.平均のバルプロ酸ナトリウム血中濃度は、68.5mg/Lであった。
プロプラノロールは28名に180 mg/d,1名に240 mg/d,3名は240
mg/dから180 mg/dに下げて使用した.
|
主要評価項目とそれに用いた統計学的手法
|
片頭痛発作頻度,1ヶ月の片頭痛のある日数.
|
結果
|
片頭痛発作頻度は,偽薬にて19%(6名)で,バルプロ酸にて66% (21名)で,プロプラノロールにて63% (20名)で減少をみた.
1ヶ月の頭痛日数に関しては,偽薬にて22% (7名),バルプロ酸にて66%
(21名),プロプラノロールにて69% (22名)で著明に減少した.
|
結論
|
前兆のない片頭痛の予防療法において,バルプロ酸とプロプラノロールでの効果に有意差はなかった.
|
作成者
|
荒木治子/竹島多賀夫
|
コメント-1
|
よくデザインされたRCT.
|
コメント-2
|
|
備考1
|
|
備考2
|
|
備考3
|
|
論文抄録
|
OBJECTIVE:
To compare the efficacy of divalproex sodium (Depakote) with that of
propranolol hydrochloride (and placebo) for the prophylaxis of migraine
without aura. DESIGN: Single-investigator, randomized, single- blind, placebo-controlled
study with 5 phases: baseline (weeks 1-4); placebo (weeks 5-8); first
treatment, 1 agent (weeks 9-20); washout (weeks 21-24); and second treatment,
crossover to other agent (weeks 25- 36). SETTING: Private practice of a
general neurologist with a special interest in headache disorders.
PATIENTS: Of 37
patients (30 women and 7 men) selected, 32 completed the study. All received
placebo, after which half were randomized to receive divalproex or
propranolol, then crossed over after washout.
INTERVENTION:
Divalproex and propranolol doses were titrated during the initial 8 weeks of
each 12-week treatment cycle. For divalproex, doses were titrated to 1500
mg/d in 23 patients, to 2000 mg/d in 2, and downward in 7; the mean valproate
sodium trough level was 68.5 mg/L. Propranolol was titrated to 180 mg/d in 28
patients, to 240 mg/d in 1, and downward in 3.
RESULTS: Migraine
frequency was reduced in 19% (6/ 32) of placebo-treated, 66% (21/32) of
divalproex-treated, and 63% (20/32) of propranolol-treated patients.
Assessment of migraine-days per month revealed significant response to
placebo in 22% (7/32) of patients, to divalproex in 66% (21/32), and to
propranolol in 69% (22/32). When results were limited to the third month of
each active-agent treatment phase, 75% (24/ 32) of patients receiving
divalproex and 78% (25/32) of those receiving propranolol had reduction in
migraine frequency.
CONCLUSION: No
significant difference was identified between divalproex and propranolol for
the prophylaxis of migraine without aura.
|
|
| |
| Diener HC, Tfelt-Hansen P, Dahlof C, Lainez MJ, Sandrini G, Wang SJ, Neto W, Vijapurkar U, Doyle A, Jacobs D; MIGR-003 Study Group: Topiramate in migraine prophylaxis--results from a placebo-controlled trial with propranolol as an active control. J Neurol 2004; 251(8): 943-950. |
文献(ABフォーム)ID
|
10
|
文献PubMed-ID
|
PMID: 15316798
|
文献タイトル(日本語)
|
片頭痛予防薬でのトピラマート--active controlとしてプロプラノロールを用いてのプラセボーコントロール試験の結果から
|
文献タイトル(英語)
|
Topiramate in migraine prophylaxis--results from a placebo-controlled trial with propranolol as an active control.
|
エビデンスレベル
|
Ib
|
著者名
|
Diener HC, Tfelt-Hansen P, Dahlöf C, Láinez MJ, Sandrini G, Wang SJ, Neto W, Vijapurkar U, Doyle A, Jacobs D; MIGR-003 Study
Group.
|
雑誌名,出版年 巻: 頁
|
J Neurol. 2004; 251(8): 943-950.
|
目的
|
To evaluate the
efficacy and safety of two doses of topiramate vs placebo for migraine prophylaxis, with propranolol (PROP) as an active control.
|
研究デザイン
|
A randomised,
double-blind, multicentre trial
|
研究施設
|
MIGR-003 Study
Group
|
研究期間
|
|
対象患者
|
Five
hundred and seventy-five subjects were enrolled from 61 centres in 13
countries.
|
介入
|
Subjects with episodic migraine with and without aura were randomised to TPM
100 mg/d, TPM 200 mg/d, PROP 160 mg/d (active control), or placebo.
|
主要評価項目とそれに用いた統計学的手法
|
The primary efficacy
measure was the change in mean monthly migraine frequency from the baseline phase relative to the double-blind treatment
phase.
|
結果
|
TPM 100 mg/d was
superior to placebo as measured by reduction in monthly migraine frequency, overall 50% responder rate,
reduction in monthly migraine days, and
reduction in the rate of daily rescue medication use. The TPM 100 mg/d and
PROP groups were similar with respect to reductions in migraine frequency, responder rate, migraine days, and
daily rescue medication usage. TPM 100 mg/d was better tolerated than TPM 200
mg/d, and was generally comparable to PROP.
|
結論
|
TPM 100 mg/d is effective in migraine prophylaxis. TPM 100 mg/d and PROP
160 mg/d exhibited similar efficacy profiles.
|
作成者
|
菊井祥二/竹島多賀夫
|
コメント-1
|
トピラマート100mg/日とプロプラノロール160mg/日は同等の片頭痛予防効果と安全性を持つ.
|
コメント-2
|
|
備考1
|
|
備考2
|
|
備考3
|
|
論文抄録
|
Topiramate (TPM) has shown efficacy in migraine prophylaxis in two large placebo-controlled,
dose-ranging trials. We conducted a randomised, double-blind, multicentre trial to evaluate the efficacy and safety of two doses
of topiramate vs placebo for migraine prophylaxis, with propranolol (PROP) as an active control.
Subjects with episodic migraine with and without
aura were randomised to TPM 100 mg/d, TPM 200 mg/d, PROP 160 mg/d (active control), or
placebo. The primary efficacy measure was the change in mean monthly migraine frequency from the baseline phase relative to
the double-blind treatment phase. Five hundred and seventy-five subjects were
enrolled from 61 centres in 13 countries. TPM 100 mg/d was superior to
placebo as measured by reduction in monthly migraine frequency, overall 50% responder rate, reduction in monthly migraine days, and reduction in the rate of daily
rescue medication use. The TPM 100 mg/d and PROP groups were similar with
respect to reductions in migraine frequency,
responder rate, migraine days, and daily rescue
medication usage. TPM 100 mg/d was better tolerated than TPM 200 mg/d, and
was generally comparable to PROP. No unusual or unexpected safety risks
emerged. These findings demonstrate that TPM 100 mg/d is effective in migraine prophylaxis. TPM 100 mg/d and PROP 160 mg/d
exhibited similar efficacy profiles.
|
|
| |
| Ziegler DK, Hurwitz A, Hassanein RS, Kodanaz HA, Preskorn SH, Mason J. Migraine prophylaxis. A comparison of propranolol and amitriptyline. Arch Neurol 1987; 44(5): 486-489. |
文献(ABフォーム)ID
|
11
|
文献PubMed-ID
|
PM: 3579659
|
文献タイトル(日本語)
|
片頭痛予防法:プロプラノロールとアミトリプチリンの比較
|
文献タイトル(英語)
|
Migraine prophylaxis. A comparison of propranolol and amitriptyline.
|
エビデンスレベル
|
Ⅰb
|
著者名
|
Ziegler DK, Hurwitz A, Hassanein RS, Kodanaz HA, Preskorn SH, Mason J
|
雑誌名,出版年 巻: 頁
|
Arch Neurol 1987; 44(5): 486-489.
|
目的
|
片頭痛予防療法にけるプロプラノロールとアミトリプチリンの有効性を比較する
|
研究デザイン
|
double-
blind, placebo-controlled, crossover design.
|
研究施設
|
|
研究期間
|
|
対象患者
|
片頭痛患者30例
|
介入
|
|
主要評価項目とそれに用いた統計学的手法
|
患者の頭痛日記から,頭痛スコアを定量し薬剤の効果を判定
受診ごとにZung,
Hamiltonの抑うつ尺度, Spielberger の不安尺度を測定.
受診ごとに薬剤投与量を増加させるかどうかを,日記をもとにコンピューターを使用して判定.
|
結果
|
プロプラノロールとアミトリプチリンは両方とも偽薬よりすぐれており,2薬剤の効果は同等であった.
薬剤の効果は,心理テストでの不安や抑うつの減少とは相関しなかった.
|
結論
|
プロプラノロールとアミトリプチリンは片頭痛の予防療法として同等に有効である.
|
作成者
|
荒木治子/竹島多賀夫
|
コメント-1
|
|
コメント-2
|
|
備考1
|
Publication Types:
·
Clinical Trial
·
Randomized Controlled Trial
|
備考2
|
|
備考3
|
The comparative efficacy of
propranolol and amitriptyline in the prophylaxis of migraine headache was
studied in 30 patients in a double- blind, placebo-controlled, crossover
design. Headache response to medication was measured monthly by compilation
of headache scores derived from quantitative data recorded by patients in a
daily diary; at each visit, Zung and Hamilton tests for depression and the
Spielberger state test for anxiety were performed. In the absence of clinical
toxicity at monthly visits, the decision to maintain the current dose or
raise it was made by a computer, which compared current headache score with
that of the previous month. Both drugs were superior to placebo. Neither drug
was superior to the other. The effectiveness of neither drug correlated with
a decrease in anxiety or depression demonstrated by psychological testing
|
|
| |
| Evers S, Afra J, Frese A, Goadsby PJ, Linde M, May A, Sandor PS: European Federation of Neurological Societies. EFNS guideline on the drug treatment of migraine--revised report of an EFNS task force. Eur J Neurol 2009; 16(9): 968-981. |
文献(ABフォーム)ID
|
12
|
文献PubMed-ID
|
PMID:
19708964
|
文献タイトル(日本語)
|
片頭痛の薬物療法に関するEFNSガイドライン-改訂版
|
文献タイトル(英語)
|
EFNS guideline on the drug treatment of migraine--revised report of an
EFNS task force.
|
エビデンスレベル
|
|
著者名
|
Evers S, Afra J, Frese A, Goadsby PJ, Linde M, May A, Sándor PS;
European Federation of Neurological Societies.
|
雑誌名,出版年 巻: 頁
|
Eur J Neurol 2009; 16(9): 968-981.
|
目的
|
文献検索と専門家委員会のコンセンサスに基づく,片頭痛の薬物療法の根拠に基づく専門家への推奨をすること。
|
研究デザイン
|
N/A
|
研究施設(セッティング)
|
N/A
|
研究期間
|
N/A
|
対象患者、サンプル数
|
N/A
|
介入
|
N/A
|
主要評価項目とそれに用いた統計学的手法
|
N/A
|
結果
|
推奨:
{片頭痛発作の急性治療}
・経口NSAIDとトリプタン
・NSAIDとトリプタンの摂取量の前に、経口メトクロプラミドまたはドンペリドン
・非常に重篤な発作において、静脈内アセチルサリチル酸または皮下スマトリプタンは、第一選択薬
・永続的に使うのはよくないが,cortoicosteroidsまたはジヒドロエルゴタミンも可能
{片頭痛の予防}
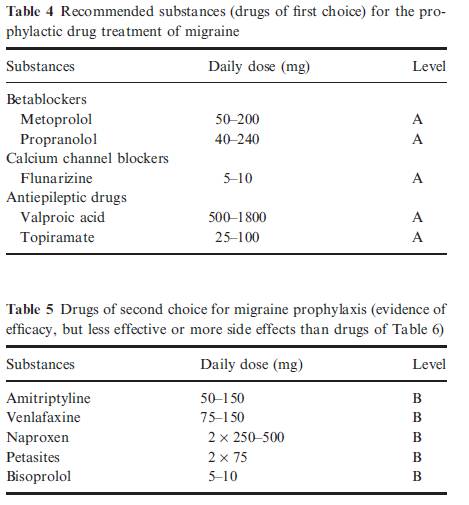
betablockers(プロプラノロールとメトプロロール),フルナリジン、バルプロ酸とトピラマートは、第一選択薬である。
第2選択薬は、アミトリプチリン、ナプロキセン、ペタサイトとビソプロロール
どのような症例に予防薬を使うか
・仕事の任務や学校の日常生活が高度に損なわれるとき。
・月当たりの発作の回数は2回以上である
・片頭痛発作は急性薬物療法に反応しないのが多い場合,非常に長い場合,不快な前兆の時.
・月当たりの片頭痛発作の頻度が3ヵ月以内に少なくとも50%減少する場合、片頭痛予防は成功と考えられる。
・治療評価のために、片頭痛ダイアリーは、有効。
第一選択の薬は、表4で示す。
第一選択薬が有効でない場合、禁忌のとき、または、患者の共存症が表5の薬に関連あるとき,第2または第3選択として推奨される
 |
結論
|
|
作成者
|
渡邉由佳/五十嵐久佳
|
コメント-1
|
|
コメント-2
|
|
備考1
|
Migraine
is one of the most frequent disabling neurological conditions with a major
impact on the patients' quality of life. To give evidence-based or expert
recommendations for the different drug treatment procedures of the different
migraine syndromes based on a literature search and an consensus in an expert
panel. All available medical reference systems were screened for all kinds of
clinical studies on migraine with and without aura and on migraine-like
syndromes. The findings in these studies were evaluated according to the
recommendations of the EFNS resulting in level A,B, or C recommendations and
good practice points. For the acute treatment of migraine attacks, oral
non-steroidal anti-inflammatory drugs (NSAIDs) and triptans are recommended.
The administration should follow the concept of stratified treatment. Before
intake of NSAIDs and triptans, oral metoclopramide or domperidon is
recommended. In very severe attacks, intravenous acetylsalicylic acid or
subcutaneous sumatriptan are drugs of first choice. A status migrainosus can
probably be treated by steroids. For the prophylaxis of migraine,
betablockers (propranolol and metoprolol), flunarizine, valproic acid, and
topiramate are drugs of first choice. Drugs of second choice for migraine
prophylaxis are amitriptyline, naproxen, petasites, and bisoprolol.
|
備考2
|
|
備考3
|
|
|
| |
| Silberstein SD: Practice parameter: evidence-based guidelines for migraine headache (an evidence-based review): report of the QualityStandards Subcommittee of the American Academy of Neurology. Neurology 2000; 55(6): 754-762. |
文献(ABフォーム)ID
|
13
|
文献PubMed-ID
|
PMID: 10993991
|
文献タイトル(日本語)
|
実地臨床パラメーター:片頭痛のエビデンスに基づくガイドライン
|
文献タイトル(英語)
|
Practice parameter:
evidence-based guidelines for migraine headache (an evidence-based review):
report of the Quality Standards Subcommittee of the American Academy of
Neurology.
|
エビデンスレベル
|
N/A
|
著者名
|
Silberstein SD.
|
雑誌名,出版年 巻: 頁
|
Neurology 2000; 55(6):
754-762.
|
目的
|
N/A
|
研究デザイン
|
4件のEBMによる片頭痛患者のマネージメントに関するレビュー1)急性期治療,2)予防療法,3)非薬物療法,4)画像検査をもとに主要な治療の勧告のみを記述.
|
研究施設
|
N/A
|
研究期間
|
N/A
|
対象患者
|
N/A
|
介入
|
N/A
|
主要評価項目とそれに用いた統計学的手法
|
N/A
|
結果
|
臨床的疑問
作成のプロセス
エビデンスの解析
片頭痛の診断
片頭痛の治療
片頭痛の急性期治療
片頭痛の予防療法
---
片頭痛予防療法の目的(ゴール):
1) 発作頻度、重症度と頭痛持続時間の軽;
2) 急性期治療の反応の改善
3)生活機能の向上と,生活への支障の軽減.
以下の項目があれば予防治療の使用を考慮する.
·
急性期の治療をしても,片頭痛発作により日常生活に支障がある場合(患者の意見による頻繁な頭痛)
·
急性期治療薬が禁忌,あるいは無効,または急性治療薬の乱用がある,急性治療による有害事象
·
急性期治療と予防療法の費用バランス
·
患者の選択(嗜好)
·
片麻痺性片頭痛、脳底片頭痛、遷延性前兆を伴う片頭痛,または片頭痛梗塞などまれな片頭痛状況の存在(神経障害の予防が必要.専門家のコンセンサスに基づく)
これらのコンセンサスに基づく片頭痛ケアの原則に従えば,予防療法が成功する可能性が高くなる.
非薬物治療も考慮すること.また,患者の選択(嗜好)も考慮が必要.
1. 薬物投与使用:
A.エビデンス基づいた有効性が最も高いレベルにある薬物の投与から予防療法を始める.
B.最低用量から開始して,有害事象が無い限り,十分な臨床効果が得られる用量までゆっくり増量する.
C.各薬剤の効果判定を十分に行う必要がある.通常,臨床効果を達成するまでに2~3ヵ月かかる可能性がある.
D.有害な薬物使用(例えば急性期治療薬の濫用)を回避する.
E.長時間作用型の製剤は、コンプライアンスを改善する可能性がある。
2. 評価:
A.頭痛日記を通して患者の頭痛をモニタする.
B.治療の再評価:3~6ヵ月後に頭痛がかなりよくコントロールされている場合、治療の漸減または、中止を考慮する.
3. 併存する医学的状態を考慮する.
いくつかの(併存症/共存しているcomorbid/coexisting)状態は、片頭痛患者において一般的である:脳卒中,心筋梗塞、Raynaud’s現象、てんかん,情動性および不安性疾患.これらの存在は,治療の機会と限界の双方に関与する.
A.可能ならば、併存症と片頭痛の双方を治療できる薬を選択する.
B.片頭痛のために使用する治療薬は,併存疾患の禁忌でないものを選択する.
C.併存症の治療に使用される薬剤は片頭痛を悪化させないものを選択する.
D.全ての薬物相互作用にも注意する.
4. 妊婦または妊娠希望の女性に対する留意点
予防的な薬物投与は、催奇形作用を持つ可能性がある。
予防療法が不可欠の場合、胎児に対するリスクが最も低い薬剤を選択する.
5. 多くの片頭痛患者は頭痛のコントロールの目的で,薬物療法の開始前,あるいは,薬物療法と同時に,非薬物療法を試みようとするものである.行動療法(Behavioral
treatments)は、3つのカテゴリーに大別できる:リラクセーション・トレーニング,バイオ・フィードバック療法,および,認知行動療法(ストレス対策トレーニング)である.
理学療法には,鍼、ervical manipulation, およびmobilization
therapyが含まれる.これらは、以下のような頭痛患者のための治療オプションである:
A.非薬物療法を好む患者
B.特異的な薬物療法に耐えれない患者
C.特異的な薬物療法が禁忌である場合
D.薬物療法に反応しない患者
E.妊婦,妊娠希望婦人,授乳婦
F.頭痛を悪化させたり,(他の薬物療法への反応性の低下を誘導する)鎮痛剤や他の急性期治療薬の長期にわたる、頻用,過剰使用のある患者(または薬剤)
G.明らかなストレス下にある患者,またはストレスのコーピング能力が不十分な患者
|
結論
|
N/A
|
作成者
|
竹島多賀夫
|
コメント-1
|
米国の片頭痛診療ガイドライン.2000年,EBMを主体にしてコンセンサスを取り入れたガイドライン.
|
コメント-2
|
|
備考1
|
Neurology55754.pdf
|
備考2
|
DA
- 20001004
IS
- 0028-3878
LA
- eng
PT
- Guideline
PT
- Journal Article
PT
- Practice Guideline
SB -
AIM
SB - IM
|
備考3
|
|
備考4
|
|
論文抄録
|
|
|
| |
| Silberstein SD, Holland S, Freitag F, Dodick DW, Argoff C, Ashman E. Evidence-based guideline update: Pharmacologic treatment for episodic migraine prevention in adults: Report of the Quality Standards Subcommittee of the American Academy of Neurology and the American Headache Society. Neurology. 2012; 78(17): 1337-1345. |
文献(ABフォーム)ID
|
14
|
文献PubMe-ID
|
PMID:225216302
|
文献タイトル(日本語)
|
エビデンスに基づくガイドラインのアップデート:成人の反復性片頭痛予防のための薬物療法
|
文献タイトル(英語)
|
Evidence-based
guideline update: Pharmacologic treatment for episodic migraine prevention in
adults: Report of the Quality Standards Subcommittee of the American Academy
of Neurology and the American Headache Society.
|
エビデンスレベル
|
N/A
|
著者名
|
Silberstein
SD, Holland S, Freitag F, Dodick DW, Argoff C, Ashman E.
Correspondence &
reprint requests to American Academy of Neurology
|
雑誌名,出版年巻: 頁
|
Neurology.
2012 Apr 24; 78(17): 1337-1345
|
目的
|
To provide updated
evidence-based recommendations for the preventive treatment of migraine
headache. The clinical question addressed was: What pharmacologic therapies
are proven effective for migraine prevention?
|
研究デザイン
|
N/A
|
研究施設
|
N/A
|
研究期間
|
N/A
|
対象患者
|
N/A
|
介入
|
N/A
|
主要評価項目とそれに用いた統計学的手法
|
N/A
|
結果
|
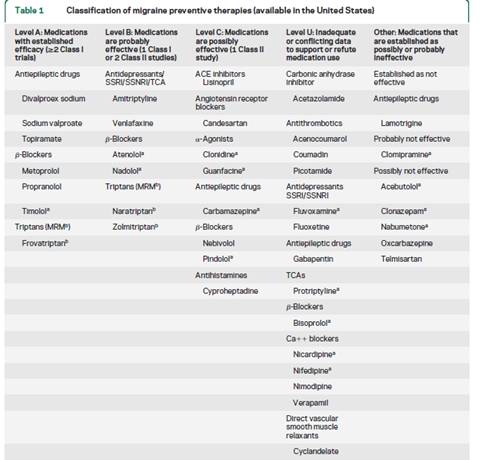
The author panel
reviewed 284 abstracts, which ultimately yielded 29 Class I or Class II
articles that are reviewed herein. Divalproex sodium, sodium valproate,
topiramate, metoprolol, propranolol, and timolol are effective for migraine
prevention and should be offered to patients with migraine to reduce migraine
attack frequency and severity (Level A). Frovatriptan is effective for
prevention of menstrual migraine (Level A). Lamotrigine is ineffective for
migraine prevention (Level A).
|
結論
|
|
作成者
|
渡邉由佳/五十嵐久佳/菊井祥二/竹島多賀夫
|
コメント-1
|
|
コメント-2
|
|
備考1
|
 |
備考2
|
|
備考3
|
|
備考4
|
|
論文抄録
|
OBJECTIVE:
To provide updated evidence-based recommendations for the preventive
treatment of migraine headache. The clinical question addressed was: What
pharmacologic therapies are proven effective for migraine prevention?
METHODS:
The authors analyzed published studies from June 1999 to May 2009 using a
structured review process to classify the evidence relative to the efficacy
of various medications available in the United States for migraine
prevention.
Results
and Recommendations: The author panel reviewed 284 abstracts, which
ultimately yielded 29 Class I or Class II articles that are reviewed herein.
Divalproex sodium, sodium valproate, topiramate, metoprolol, propranolol, and
timolol are effective for migraine prevention and should be offered to
patients with migraine to reduce migraine attack frequency and severity
(Level A). Frovatriptan is effective for prevention of menstrual migraine
(Level A). Lamotrigine is ineffective for migraine prevention (Level A).
|
|
| |